Use the following links to jump directly to the Chapter you'd like to view:
Chapter 1 Chapter 2 Chapter 3Chapter 1
THE FAILURE OF THE REASONABLENESS TEST CRITERIA REVIEW PROCESS TO RESOLVE DEFERRED CLAIMS HELPED EXPOSE FLAWS IN THE ADMINISTRATION OF THE SCHOOL-BASED MEDI-CAL ADMINISTRATIVE ACTIVITIES PROGRAM
Chapter Summary
The California Department of Health Care Services (Health Care Services) implemented the claims review process involving reasonableness test criteria in response to a financial management review that the federal Centers for Medicare and Medicaid Services (CMS) conducted on California’s School-Based Medi-Cal Administrative Activities program (administrative activities program). We believe that this claims review process was reasonable and would have maximized federal reimbursements to the claiming units if Health Care Services had accurately communicated and applied the criteria and if claiming units had complied with the process’s CMS-approved requirements.8 However, as executed, this process failed to result in Health Care Services’ approval of many deferred claims. In addition, local educational consortia and local governmental agencies approved and forwarded claims that Health Care Services did not approve as complying with the process’s requirements.9 Therefore, we believe that local educational consortia and local governmental agencies provided little value during this process. In addition, Health Care Services has no formal appeals process available for claiming units wishing to directly appeal its decisions to not approve reimbursement claims filed under the process.
Furthermore, Health Care Services does not effectively oversee the local educational consortia and local governmental agencies with which it contracts to perform key administrative and oversight functions for the administrative activities program. For example, Health Care Services’ lack of oversight prevents it from detecting unallowable provisions in the contracts between local educational consortia or local governmental agencies and their claiming units.
Health Care Services’ Claims Review Process Involving Reasonableness Test Criteria Failed to Result in the Payment of Many Deferred Claims
Health Care Services’ reasonableness test criteria review process for the administrative activities program failed to result in the approval of many deferred claims. As shown in Table 3, Health Care Services approved fewer than 10 percent of the reimbursement claims that claiming units submitted during the nearly one-year period under this process, and it did not review all of the claims it received before the reasonable test criteria process was cancelled. Consequently, claiming units received very few federal reimbursements through this process. Despite the low number of approved reimbursement claims, we believe that this process would have maximized federal reimbursements to claiming units if Health Care Services had accurately communicated and applied the criteria and if the claiming units had complied with the process’s CMS-approved requirements.
As described in the Introduction, Health Care Services’ implementation of the reasonableness test criteria flowed out of a recommendation from CMS’s financial management review. CMS instructed Health Care Services to implement a reasonableness review to ensure that claims and time studies were reasonable and that proper time coding was used. Using the Kern County Office of Education (Kern County) methodology as a model, CMS recommended that Health Care Services develop its reasonableness test criteria based on authorized job classifications, claiming data, and vendor fee limits. The Kern County methodology was chosen because CMS did not have to defer payments for reimbursement claims for the Santa Barbara County Education Office–Special Education Division (Santa Barbara), which submitted its claims through the four-county local educational consortium led by Kern County. During its financial management review, CMS had reviewed the time survey results for one of Santa Barbara’s quarterly claims and interviewed time study participants and representatives from Kern County, and it determined that the time survey results for the individual participants were reasonable given their job responsibilities and that Kern County had performed a thorough review of the claim including assessing the reasonableness of both the time study results and other direct charges reported on the claim. Based on this review, CMS validated that all claimed costs for Santa Barbara for fiscal year 2010–11 met federal requirements and it concluded that Santa Barbara was administering the time study and completing claims in accordance with the approved school-based administrative claiming guide.10
Table 3
Approval Rates for Reimbursement Claims Submitted Under the Reasonableness Test Criteria Review Process, Which Was in Place From October 28, 2013, Through October 7, 2014
| NAME OF LOCAL ENTITY | NUMBER OF CLAIMS SUBMITTED | NUMBER OF CLAIMS APPROVED FOR PAYMENT | DOLLAR AMOUNT OF CLAIMS SUBMITTED | DOLLAR AMOUNT OF CLAIMS APPROVED FOR PAYMENT | PERCENTAGE OF CLAIMS APPROVED FOR PAYMENT |
|---|---|---|---|---|---|
Local educational consortium | |||||
Region 1—Sonoma County Office of Education |
|||||
| Region 2—Glenn County Office of Education | |||||
| Region 3—Sutter County Superintendent of Schools Office | |||||
| Region 4—Contra Costa County Office of Education | |||||
| Region 5—Santa Cruz County Office of Education | |||||
| Region 6—Stanislaus County Office of Education | |||||
| Region 7—Madera County Office of Education | |||||
| Region 8—Kern County Office of Education | |||||
| Region 9—Orange County Department of Education | |||||
| Region 10—San Bernardino County Superintendent of Schools | |||||
| Region 11—Los Angeles County Office of Education | |||||
| Subtotals | |||||
Local governmental agency* |
|||||
| Alameda County Health Care Services Agency | |||||
| Fresno County Auditor-Controller/Treasurer-Tax Collector | |||||
| Imperial County Public Health Department | |||||
| Inyo County Health and Human Services | |||||
| Kern County Department of Public Health | |||||
| Riverside County Fiscal Services—Community Health Agency | |||||
| Sacramento County Health and Human Services | |||||
| San Bernardino County Department of Aging and Adult Services | |||||
| San Diego County Health and Human Services Agency | |||||
| City and County of San Francisco Department of Public Health | |||||
| San Luis Obispo County Public Health Department | |||||
| Santa Clara County Finance/Public Health | |||||
| Solano County Health and Social Services Department | |||||
| Tulare County Health and Human Services Agency | |||||
| City of Pasadena Public Health Department | |||||
| Subtotals | |||||
| Totals | |||||
Sources: The School-Based Medi-Cal Administrative Activities Interim Claiming and Reasonableness Test Criteria Tracker database, and the California Department of Health Care Services’ (Health Care Services) and local governmental agency consortium’s websites. See the Methods Used to Assess Data Reliability section in the Introduction to the report regarding the electronic data used in the table.
Note: This table shows the number of claims that Health Care Services received and approved under the reasonableness test criteria. However, Health Care Services did not review an unknown number of claims before it discontinued the process.
* These local governmental agencies serviced claiming units in their respective regions when the latter submitted the listed claims.
Furthermore, according to its documentation, when developing the reasonableness test criteria, Health Care Services consulted with CMS to develop statewide standards for each type of administrative activity. For example, Health Care Services developed limits on the overall percentage of time that each claiming unit’s time survey participants spent on administrative activities in relation to their total work time that could be included in claims for federal reimbursement. Health Care Services also limited the number of administrative staff that could participate in the time survey and the amount of external vendor fees that could be included in reimbursement claims. See Table 4 for a summary of the reasonableness test criteria.
Health Care Services recognized that each local educational agency is unique and represents a unique set of circumstances, and it set up an exception component to the reasonableness test criteria, which CMS approved as part of the process. Under the new process, Health Care Services would allow claiming units to exceed or otherwise not comply with the benchmark percentages, limits, or authorized time survey participants if the claiming units submitted an adequate justification why exceeding the criteria was reasonable and necessary for the proper and efficient administration of the Medi-Cal program. Health Care Services also developed and posted on its website several example justifications to help local educational agencies prepare their own. For instance, Health Care Services used one of these examples to illustrate an adequate justification for a fictitious school district whose time study participants spent 4.63 percent of their overall time on initial Medi-Cal outreach (which exceeded the 4 percent limit for this activity). In the example, the fictitious school district successfully justified exceeding the limit for this administrative activity by explaining that a high percentage (68 percent) of its large student population is eligible for Medi-Cal and its community service workers serve a vital role in connecting these students with programs and services related to Medi-Cal. Because community service workers perform a heavy volume of daily work related to Medi-Cal, a substantial portion of their time would therefore be reasonably allotted to reimbursable Medi-Cal outreach activities.
Table 4
California Department of Health Care Services’ Reasonableness Test Criteria
The California Department of Health Care Services (Health Care Services) required claiming units to take the following actions to obtain approval of deferred claims under the reasonableness test criteria review process for the School-Based Medi-Cal Administrative Activities program:
- Remove all unauthorized job classifications from the time study.
- Limit clerical and administrative positions to no more than 20 percent of the total number of nonclerical and nonadministrative time study participants.
- Limit vendor fees to 15 percent of the total amount of the claim (after the application of other reasonableness test criteria).
- Apply the following percentage limits to the overall time survey results (which indicate the percentage of time that participants spent on various administrative activities during the survey period) for each billable administrative activity:
| ADMINISTRATIVE ACTIVITY | LIMIT |
|---|---|
| Medi-Cal outreach | |
| Facilitating Medi-Cal applications | |
| Referral, coordination, and monitoring of Medi-Cal services 8 | |
| Arranging transportation to support Medi-Cal services | |
| Translation of documents related to Medi-Cal services | |
| Program planning, policy development, and interagency coordination related to Medi-Cal services |
|
| Medi-Cal claims administration, coordination, and training | |
| General administration, completing the time survey form, and paid time off† |
Sources: Health Care Services’ Policy and Procedure Letter 13-012, its California School-Based Medi-Cal Administrative Activities Manual, and interviews with Health Care Services’ staff.
Note: If a claim is not in compliance with the above limits (with the exception of the limits related to vendor fees), claiming units could submit a written justification to Health Care Services explaining the reasons for the noncompliance.
* For fiscal year 2012–13 and later, Health Care Services increased the limit on Medi-Cal claims administration, coordination, and training from 4 percent to 7 percent, and decreased the limit on general administration, completing the time survey form, and paid time off from 10 percent to 7 percent.
† General administration, completing the Medi-Cal administrative activities time survey form, and paid time off are allocated to other activities.
The reasonableness test criteria that Health Care Services developed were not inconsistent with federal requirements. Federal requirements specify that all costs submitted for reimbursement must be “necessary and reasonable for the proper and efficient performance and administration of federal awards.” As we mentioned earlier, CMS required Health Care Services to implement a reasonableness review process. CMS also approved the benchmarks and other criteria that Health Care Services established for this process. Given that CMS directed Health Care Services to develop and implement a reasonable process for reviewing reimbursement claims, that Health Care Services created the reasonableness test criteria using Kern County’s methodology as a starting point as CMS recommended, and that CMS approved the criteria that Health Care Services proposed, we believe that the reasonableness test criteria including the benchmark percentages and other limits it established were in themselves reasonable.
Health Care Services used a checklist to log compliance with the benchmark percentages and other criteria to document its review of claims that claiming units submitted under the process. Health Care Services also reviewed the documentation that claiming units included in their claims to ensure that no staff positions were reporting an unreasonable amount of time spent on Medi-Cal administrative activities in relation to time spent on their other responsibilities. As explained in Table 1 earlier, we reviewed 10 reimbursement claims to determine whether Health Care Services had effective fiscal and administrative controls over the reasonableness test criteria review process to ensure that local educational agencies received consistent, appropriate, and timely reimbursements. We also determined whether the process for reimbursements was consistently applied across all local educational agencies. Health Care Services approved only three of the 10 claims. Of those three, one complied with the benchmarks and other criteria, and Health Care Services concluded that another included an acceptable justification for exceeding various benchmarks. Health Care Services acted leniently in approving the third claim because, although it concluded that two of the three justifications for noncompliance with various benchmarks were not reasonable, it approved the claim anyway, citing the claiming unit’s small size of the time survey participant pool and the minimal degree of the overages. Health Care Services did not approve the other seven claims because they exceeded the benchmarks or included unauthorized positions in their time studies without adequate justifications, included excessive vendor fees, did not include adequate supporting documentation, or the individual positions reported unreasonable amounts of time spent on Medi-Cal administrative activities. Based on our review of these seven claims, we believe that Health Care Services’ decision not to approve them was reasonable.
However, in reviewing the 10 claims, we found that Health Care Services’ controls over the reasonableness test criteria review process were insufficient to ensure consistent, appropriate, and timely federal reimbursements. Health Care Services issued a policy and procedure letter in October 2013 to notify stakeholders of the new reasonableness test criteria, in which it specified the benchmarks and other criteria with which claiming units had to comply. However, we found that this letter included inaccurate benchmarks related to two administrative categories. As shown in Table 4, Health Care Services increased the time limit on Medi-Cal claims for administration, coordination, and training from 4 percent to 7 percent, and decreased the time limit on general administration, completing the time survey form, and paid time off from 10 percent to 7 percent for all claims related to fiscal year 2012–13 and later. Health Care Services’ chief of its Medi-Cal Administrative Claiming Section (section chief) told us that the changes were due to revisions made to its California School-Based Medi-Cal Administrative Activities Manual (manual) between fiscal years 2011–12 and 2012–13 to move time spent completing the time survey from one activity category to another. However, she stated that she did not have any documentation showing that Health Care Services relayed this change in criteria to the local educational consortia, local governmental agencies, or local educational agencies. Neither the initial 2013 policy and procedure letter sent to stakeholders nor another letter describing the reasonableness test criteria that was updated in April 2014 included the updated benchmarks for these two categories. Consequently, some claiming units may have believed that their claims complied with the reasonable test criteria only to have Health Care Services conditionally deny their claims because Health Care Services was using the revised benchmarks and the claiming units were not. We also found that three of the 10 checklists that we reviewed did not contain the right benchmarks for these two categories of activities based on the period of the claim. Although Health Care Services’ use of the wrong benchmarks did not result in improper decisions for these three claims, it is conceivable that it may have made improper decisions to approve or not approve other claims because its claim reviewers were using the wrong benchmarks for these two activity categories. Because Health Care Services did not accurately communicate the reasonableness test criteria to stakeholders and because it sometimes used incorrect criteria when reviewing claims, we believe it contributed to the failure of the reasonableness test criteria process to result in the payment of many deferred claims.
Health Care Services Has Offered Claiming Units No Formal Opportunity to Appeal Its Decisions to Deny Reimbursement Claims
Health Care Services has had no processes in place that allow claiming units to directly appeal its decisions to not approve claims submitted under the reasonableness test criteria review process. Health Care Services’ manual allows local educational consortia and local governmental agencies to request that Health Care Services reconsider such decisions. However, neither state law nor Health Care Services’ manual identifies claiming units as entities that can directly appeal Health Care Services’ decisions. According to the chief of the Safety Net Financing Division, local educational consortia or local governmental agencies can appeal Health Care Services’ actions or decisions, such as denying claims, on behalf of their claiming units.
Health Care Services has a formal appeals process that allows claiming units to appeal actions or decisions that local educational consortia or local governmental agencies make but not decisions that Health Care Services makes. In April 2014 Health Care Services issued a policy and procedure letter that established a formal process for local educational agencies to appeal actions or decisions that local educational consortia or local governmental agencies made. This letter instructed local educational agencies on how to file a request for appeal to Health Care Services within six months of an unresolved or disputed decision or action. According to the policy, Health Care Services would then generally provide a written decision to all parties within 90 days. According to the assistant chief of the Safety Net Financing Division (assistant division chief), no claiming units have ever used this formal appeals process. We believe that Health Care Services should revise its appeals process to allow claiming units to directly appeal its decisions since these decisions likely have more of a financial impact on the claiming units than on the local educational consortia and local governmental agencies that represent them.
Local Entities Added Little Value When They Reviewed Claims Using Reasonableness Test Criteria
We observed that local educational consortia and local governmental agencies appeared to add little value during the reasonableness test criteria review process. In its policy and procedure letter initiating that process, Health Care Services instructed local educational consortia and local governmental agencies to “review and forward” reimbursement claims to it. We asked Health Care Services to clarify for us what this instruction meant, and the assistant division chief told us it expected those entities to reject claims that failed to meet the reasonableness test criteria and that did not contain adequate justification for noncompliance. In addition, staff at the claiming units’ local educational consortium or local governmental agency signed a statement on each reimbursement claim certifying that the information provided was true and correct, was based on actual expenditures of the claiming unit, was necessary for federal matching funds according to federal regulations, and was for allowable administrative activities. Despite these factors, it does not appear that these entities properly reviewed claims submissions because many of these claims did not conform to the reasonableness test criteria.
Although Health Care Services did not review all claims it received while the reasonableness test criteria review process was in effect, for the claims it did review, it conditionally denied more than two and a half claims for each one it approved. During our review of 10 claims described earlier, we noted instances where local educational consortia or local governmental agencies approved claims that did not comply with the reasonableness test criteria benchmarks or other criteria and that did not contain adequate justifications. To determine whether these were isolated occurrences, we examined additional claims at Health Care Services. We identified an additional 10 claims that local educational consortia or local governmental agencies approved and forwarded to Health Care Services that did not contain required justifications. Further, before the implementation of the reasonableness test criteria review process, CMS found in its financial management review that instead of providing consistent oversight and monitoring guidance to claiming units, local educational consortia and local governmental agencies either established their own standards or performed a very cursory review of the claiming units’ submissions. In general, our findings mirrored the results of CMS’s review.
When we questioned Health Care Services about why it did not take adverse action against local educational consortia and local governmental agencies when they continued to forward unallowable claims, the assistant division chief told us that the reasonableness test criteria review process was new for all parties and that it was working collaboratively with the local educational consortia and local governmental agencies to ensure that they understood the process and that it viewed this as an educational opportunity rather than a punitive one.
Health Care Services Has Not Effectively Overseen Local Educational Consortia and Local Governmental Agencies in the Past
Health Care Services has an established record of failing to monitor local educational consortia and local governmental agencies. Federal requirements charge Health Care Services, as California’s single state agency responsible for Medicaid, with supervising and administering the administrative activities program. As our Introduction notes, Health Care Services contracts with local educational consortia and local governmental agencies to perform key administrative and oversight functions for the administrative activities program, which in turn contract with the claiming units. The responsibilities of the local educational consortia and local governmental agencies include training claiming unit staff, overseeing the time survey process, and reviewing and submitting reimbursement claims to Health Care Services on behalf of participating claiming units. Health Care Services’ policy requires it to monitor every local educational consortium and local governmental agency at least once every three years.
Reports citing oversight concerns include an audit that the California State Auditor released in August 2005. In that audit report titled Department of Health Services: Participation in the School-Based Medi-Cal Administrative Activities Program Has Increased, but School Districts Are Still Losing Millions Each Year in Federal Reimbursements (report number 2004-125), we noted that Health Care Services did not conduct a sufficient number of site visits to local educational consortia and local governmental agencies. We concluded that this lack of oversight meant that Health Care Services was unable to ensure that local educational consortia and local governmental agencies were properly administering the administrative activities program.
More recently, the annual federal compliance reports that we issued covering the state fiscal years ending in June 2012, 2013, and 2014 all pointed out that Health Care Services had not conducted site or desk reviews of local educational consortia and local governmental agencies within the required time frame. These reports, required by state law, assess the State’s compliance with federal laws and regulations. In fiscal year 2011–12, Health Care Services did not perform site or desk reviews on seven of the 28 local educational consortia and local governmental agencies participating in the administrative activities program. Health Care Services attributed this backlog to a ban on discretionary travel instituted in 2011, but it stated that it would complete the reviews by June 30, 2013. However, the following year, the number of reviews it failed to conduct increased from seven to nine. Health Care Services again attributed the cause to the 2011 travel restrictions, plus the CMS financial management review and the development of the new claiming plan. Health Care Services stated this time that it anticipated completing the overdue site visits or desk reviews by June 30, 2014. Nevertheless, by the end of fiscal year 2013–14, the number of reviews it had failed to conduct had grown to 15, and Health Care Services offered no explanation in its response to this report other than to say that it was reviewing site visit requirements and expected to begin site visits in spring 2015. However, according to the section chief, Health Care Services now plans to commence site visits in August 2015. This lack of adequate monitoring increases the risk that local educational consortia and local governmental agencies are not performing the oversight and administrative tasks for which they are responsible.
Because of its continued inability to conduct desk or site reviews with reasonable frequency, we believe Health Care Services could monitor program participants more cost-effectively if it were to employ a risk-based approach as do other states we reviewed for this audit. Health Care Services’ process for reviewing local educational consortia and local governmental agencies consists of a detailed review of the documentation to support two fiscal years’ worth of invoices for two claiming units once every three years. More specifically, Health Care Services is supposed to review each entity at least once every three years regardless of other factors.
In contrast to Health Care Services’ attempt to monitor local educational consortia and local governmental agencies according to a set schedule, the Medicaid agencies for Illinois and Michigan use a risk-based approach and consider various risk factors when selecting and scheduling program participants for review. For example, Michigan considers risk factors that include the dollar amount of claims, the existence of previous audit findings, and turnover of key claiming unit staff. Using a risk-based approach to select and review participants helps these states focus their limited monitoring resources on those participants that are most likely to have problems or that are most likely to have findings with the biggest impact on the program. We believe that if Health Care Services used a risk-based strategy to select and review participants, it would, similarly, be better able to focus its resources on monitoring the riskier participants with which it contracts.
Health Care Services Continues to Ineffectively Oversee the Medi-Cal Administrative Activities Program
Despite the findings and recommendations cited in prior audits and Health Care Services’ repeated assurances that it would address the audits’ findings, certain weaknesses in its oversight of local educational consortia and local governmental agencies remain. These flaws reduce the likelihood that claimed costs will be reasonable and necessary, and that they will therefore qualify for federal reimbursement. For instance, the contract issued by one local educational consortium with about 80 claiming units participating in the administrative activities program, including the State’s largest claiming unit—the Los Angeles Unified School District (LA Unified)— could inappropriately allow those claiming units to claim costs that Health Care Services has already claimed. Federal regulations generally allow California entities to receive federal reimbursement of up to 50 percent of the costs they incur for the administrative activities program. Health Care Services claims federal reimbursement for 50 percent of the costs for its administration of the administrative activities program. It then passes on the other 50 percent of its costs to the local educational consortia and local governmental agencies in the form of a participation fee. Because Health Care Services already claimed reimbursement from the federal government for 50 percent of its costs, other entities are prohibited from including Health Care Services’ participation fee as part of their own claim for federal reimbursement. Otherwise, the federal government could end up paying more than 50 percent of Health Care Services’ costs.
Nevertheless, the Los Angeles County Office of Education (Los Angeles County) passes on Health Care Services’ participation fee to its claiming units. According to the terms of the contract between Los Angeles County and its claiming units, claiming units are allowed to include the participation fee as part of the costs in their reimbursement claims. As a result of these contract provisions, LA Unified submitted at least one claim that included unallowable charges. Presumably many of the invoices that Los Angeles County has submitted on behalf of its claiming units contain similar unallowable charges. According to its manager of business advisory services, Los Angeles County was not aware that Health Care Services claims federal reimbursement for its costs. In addition, he stated that Los Angeles County will review its records to identify invoices that contained Health Care Services’ participation fee and refund any unallowable charges as appropriate.
Contracts between local educational consortia and local governmental agencies and their claiming units contain problematic provisions, in part, because Health Care Services does not monitor the contracts and is unaware of any contract weaknesses. Health Care Services’ manual states that Health Care Services expects the language in these contracts to “mirror” the language in the contracts between Health Care Services and the local educational consortia and local governmental agencies. However, Health Care Services does not dictate the terms of or maintain copies of the contracts between local educational consortia or local governmental agencies and their respective claiming units. The assistant division chief stated that Health Care Services includes these contracts as part of the desk or site review process. Nevertheless, the review to which the assistant division chief refers checks only to ensure that the claiming unit is not claiming a fee based on a percentage of the federal reimbursement, that the contract was in effect on the date of the claim, and that the reimbursable administrative activities listed in the contract match what is in the manual. According to an assistant chief counsel for Health Care Services, it would have the ability to dictate the terms of contracts between claiming units and local educational consortia and local governmental agencies if there was a regulation, but there are no regulations on this point. However, as California’s single state agency for Medicaid and the administrative activities program administrator, Health Care Services should ensure that all interagency agreements related to Medi-Cal are consistent with federal requirements and that claims are allowable. We further discuss Health Care Services’ lack of regulations in Chapter 3.
Another contract weakness relates to the payment provisions contained in contracts between some local educational consortia and local governmental agencies and their claiming units. Federal guidance urges caution when program participants, which would include claiming units, pay for professional services based on percentages of the reimbursement because it may increase the risk of abusive billing practices. Before Health Care Services implemented the random moment time survey methodology, the local educational consortia and local governmental agencies were responsible for ensuring the accuracy and reasonableness of claiming units’ reimbursement claims. However, some local educational consortia and local governmental agencies charge claiming units a percentage of their reimbursement. As such, the higher the approved reimbursement amount, the more the local educational consortium or local governmental agency could retain as payment.
Such payment provisions unnecessarily increase the risk that these local educational consortia and local governmental agencies might approve otherwise unallowable reimbursement claims to increase the revenue they earn from claiming units. Furthermore, local educational consortia and the local governmental agencies do not bear the primary financial risk associated with reimbursements that are subsequently disallowed based on audits or other reviews; instead, the claiming units do. Claiming units are financially responsible for paying back federal reimbursements that audits or similar reviews identify as unallowable, not the local educational consortia and local governmental agencies. It is currently unclear whether local educational consortia or local governmental agencies would have to return administrative fees to claiming units that were contingent on reimbursements that were subsequently disallowed.
We noted a similar concern associated with the random moment time survey. According to the section chief, local educational consortia elected to use in-house staff to code the time survey responses as opposed to hiring a third-party vendor. According to Health Care Services’ documentation, as of April 2015 eight of the 11 local educational consortia charge their claiming units administrative fees based upon a percentage of their reimbursements. The decisions the coders make can directly affect the amount of compensation that the local educational consortium will receive, and this increases the risk that they will improperly code time survey responses as reimbursable activities. In fact, stakeholders raised similar concerns that if local educational consortia and local governmental agencies code survey responses, prepare invoices, and monitor claiming units, it may result in conflicts of interest. In contrast, California’s local governmental agency consortium (all but San Diego County), Illinois, Michigan, and Texas all hired vendors to code their time survey responses that are not paid based on a percentage of their reimbursement. Because the vendors’ compensation is not tied to the amount of the reimbursement, they have no financial incentive to code more survey responses as reimbursable activities.
Health Care Services could ensure that the contracts with claiming units for the administrative activities program are appropriate and consistent with state and federal requirements by contracting directly with claiming units using a standardized contract. The Medicaid agencies in both Illinois and Texas contract directly with claiming units that wish to claim federal reimbursements for their respective administrative activities programs. Contracting directly with the school districts helps ensure that the districts have consistent contract language to follow to avoid unallowable costs. In fact, the Texas Medicaid agency publishes a standard contract for its administrative activities program online and it directs claiming units to download, print, sign, and submit the contract. Because this contract is standardized—that is, claiming units have no ability to modify its terms—the Texas Medicaid agency can ensure that these contracts are consistent and comply with applicable federal and state requirements. Similarly, Health Care Services publishes a standardized contract for the Local Educational Agency Medi-Cal Billing Option Program (billing option program) on its website to help ensure compliance with state and federal requirements. Local educational agencies must sign this contract if they intend to participate in the billing option program.
The lack of fiscal transparency of the costs and revenues of local educational consortia and local governmental agencies is another area where Health Care Services’ oversight falls short. Not only do federal regulations require that claiming units claim only those costs that are reasonable and necessary for the proper and efficient administration of the program, but those regulations also prohibit program participants from earning a profit from administering the administrative activities program. Health Care Services allows local educational consortia and local governmental agencies to charge claiming units an administrative fee to help cover the costs they incur to administer the program. Depending on the local educational consortium or local governmental agency, this fee may be a percentage of the claiming unit’s reimbursement, a portion of the actual costs of the local educational consortium or local governmental agency, a per-participant fee, or a fee based on the claiming unit’s student enrollment. Health Care Services does not require local educational consortia and local governmental agencies to report how much they collect in administrative fees from claiming units. Because it does not collect this information, Health Care Services cannot determine if the local educational consortia or local governmental agencies are collecting administrative fees in excess of their costs, which would result in an inappropriate profit and an unnecessary financial expense for claiming units. Further, because it does not track or report this financial information, Health Care Services cannot ensure that these administrative fees are reasonable and necessary and therefore allowable as federal regulations require. Finally, this lack of fiscal transparency prevents Health Care Services from determining if claiming units are paying an excessive portion of their reimbursements to their respective local educational consortia or local governmental agencies.
Other states’ administrative activities programs provide greater fiscal transparency. Claiming units in both Illinois and Texas submit claims directly to the state, and the states withhold 4 percent and 5 percent of the reimbursement, respectively, to defray the cost of administering the program. Illinois and Texas have no intermediate parties such as local educational consortia or local governmental agencies and their claiming units can easily determine how much of their reimbursement they will retain without needing additional fiscal reporting. In addition, the Michigan Medicaid agency publishes annually a document on its website that shows the cost of its statewide random moment time study and claim calculation process, including vendor fees for its administrative activities program. The document also shows each intermediate school district’s share of the cost.11 Health Care Services could enhance the fiscal transparency of its administrative activities program by adopting and then adapting these other states’ practices for use in California.
We were also asked to compare the extent to which other states’ and California’s reporting requirements allow for tracking student outcomes. However, it does not appear that state Medicaid programs are tracking this information. For example, the director of cost reporting, time study, and data support services at the Texas Medicaid agency is not aware of any requirement that the Medicaid agency track or report student outcomes. Similarly, a public service administrator from the Illinois Medicaid agency stated that it does not track any student outcome information other than Medicaid enrollment. Health Care Services’ section chief also informed us that she is not aware of any requirement to track student outcomes and that Health Care Services does not currently do so.
Recommendations
To ensure that Health Care Services provides claiming units with reasonable opportunities to address concerns with its decisions or actions, it should take the following actions within three months:
- Begin preparing regulations to establish and implement a formal appeals process that allows claiming units to directly appeal Health Care Services’ decisions.
- Inform all stakeholders, including claiming units, of the existence of this appeals process.
Until the Legislature implements our recommendation in Chapter 2, Health Care Services should immediately resolve weaknesses in its oversight of local educational consortia and local governmental agencies to ensure that these entities sufficiently meet their responsibilities under the administrative activities program and meet the terms of their contracts with Health Care Services. Actions to take include the following:
- Update its site review and desk review procedures to include the following steps:
- A risk-based approach to selecting entities for review.
- Verification that local educational consortia and local governmental agencies are adequately meeting the oversight and administrative responsibilities described in their contracts with Health Care Services.
- Verification that contracts between local educational consortia or local governmental agencies and their claiming units do not include provisions that could result in disallowed costs, such as allowing Health Care Services’ participation fee to be included in the claim calculations.
- Examination of local educational consortia and local governmental agencies’ records to ensure that:
- Costs they claim for federal reimbursement are necessary and reasonable.
- The entities are not inappropriately earning a profit based on the fees they collect from claiming units.
- The coding performed by local educational consortia that charge claiming units a percentage of their federal reimbursement is reasonably accurate.
- Complete the oversight reviews for at least three high-risk local educational consortia or local governmental agencies by December 31, 2015, and post the results to its website.
- Complete the oversight reviews for any remaining high-risk local educational consortia or local governmental agencies by June 30, 2016, and post the results to its website.
To minimize the risk that claiming units could include unallowable costs when calculating their reimbursement claims, Health Care Services should take the following actions immediately:
- Encourage Los Angeles County to revise its contracts with its claiming units to make it clear that claiming units cannot include Health Care Services’ participation fee as part of their claims.
- For all claims that Los Angeles County received and reviewed under its current contracts with its claiming units, Health Care Services should do the following:
- Determine whether claiming units included Health Care Services’ participation fee as part of the claim.
- For those paid claims that included the participation fee, identify the inappropriate amount paid and take appropriate action to resolve the improper payment including, if necessary, obtaining a refund from the claiming unit.
- For those submitted claims that have not yet been paid, instruct Los Angeles County to reject the claims and direct claiming units to revise the claims to omit Health Care Services’ participation fee.
- Remind all local educational consortia and local governmental agencies that contracts with their claiming units should prohibit claiming units from seeking federal reimbursement of Health Care Services’ participation fee.
Chapter 2
IMPLEMENTING A SINGLE STATEWIDE TIME SURVEY WOULD BE MORE COST-EFFECTIVE THAN THE CALIFORNIA DEPARTMENT OF HEALTH CARE SERVICES’ CURRENT APPROACH TO ESTIMATING MEDI-CAL ADMINISTRATIVE TIME
Chapter Summary
When it implemented the random moment time survey methodology, the California Department of Health Care Services (Health Care Services) missed an opportunity to implement a statewide quarterly time survey for the School-Based Medi-Cal Administrative Activities program (administrative activities program). Random moment time surveys are used to estimate the portion of time that participating staff spend on reimbursable administrative activities during a given quarter. Health Care Services could have implemented a single statewide survey but did not. Instead, local educational consortia, local governmental agencies, and the Los Angeles Unified School District (LA Unified) conduct nine different time surveys each quarter.12,13
As discussed in the Introduction, state law currently requires claiming units to submit claims through either a local educational consortium or local governmental agency.14 However, a single statewide time survey could render the local educational consortia and local governmental agencies’ involvement in the administrative activities program unnecessary. We identified two states—Illinois and Texas—that each implemented a single statewide survey and no longer include consortia of school districts in their programs. The costs associated with implementing and conducting nine surveys rather than a single statewide survey are considerable and are neither necessary nor efficient. Health Care Services did not implement the single survey itself because it did not believe it had the time to acquire the necessary software. Also, Health Care Services did not require local educational consortia and local governmental agencies to minimize the cost and administrative burdens associated with the surveys. By switching to a single statewide survey, Health Care Services could reduce the number of survey notifications per quarter to only 5,522 rather than the 49,698 under the current nine-survey structure. Having fewer survey responses would result in lower administrative costs to review survey responses and to ask clarifying questions. Finally, because of the process that Health Care Services used to issue interim payments, some claiming units may not receive the full interim payments to which they are entitled under the settlement agreement with CMS.
Health Care Services Could Reduce California’s Medicaid Program Costs by Conducting One Statewide Survey
When Health Care Services implemented the random moment time survey methodology for its administrative activities program, it missed an opportunity to implement a single statewide quarterly time survey. Random moment time surveys are used to estimate the portion of time that participating staff spend on reimbursable administrative activities during a given quarter. Health Care Services’ use of a single quarterly time survey throughout the State would have minimized costs for claiming units—the school districts or local educational programs that claim reimbursements for participating in the administrative activities program—and for the federal government. Federal regulations require that all costs claimed and submitted to the federal government for federal programs be necessary and reasonable for the program’s efficient operation. Because Health Care Services had the opportunity to implement a single statewide quarterly time survey that could have saved money for stakeholders, the costs and effort associated with implementing nine different quarterly time surveys by local educational consortia, local governmental agencies, and LA Unified are neither necessary nor efficient.
Moreover, Health Care Services delegated the responsibility for implementing the random moment time survey methodology to the local educational consortia and local governmental agencies. Although CMS approved Health Care Services’ implementation of the new time survey methodology, according to a CMS representative, it was not involved in the decision to have separate time surveys in multiple geographic regions around the State. When they kicked off the new methodology in January 2015, the local educational consortia and local governmental agencies conducted separate quarterly time surveys covering different geographic regions, plus the preexisting one conducted by LA Unified. Health Care Services refers to the nine entities that generate the random moments for these quarterly time surveys as administrative units. Figure 4 summarizes the entities involved in issuing the nine quarterly surveys and proposes a more streamlined alternative structure.
Figure 4
California’s Current Time Survey Structure for the School-Based Medi-Cal Administrative Activities Program and a Proposed Revision to That Structure
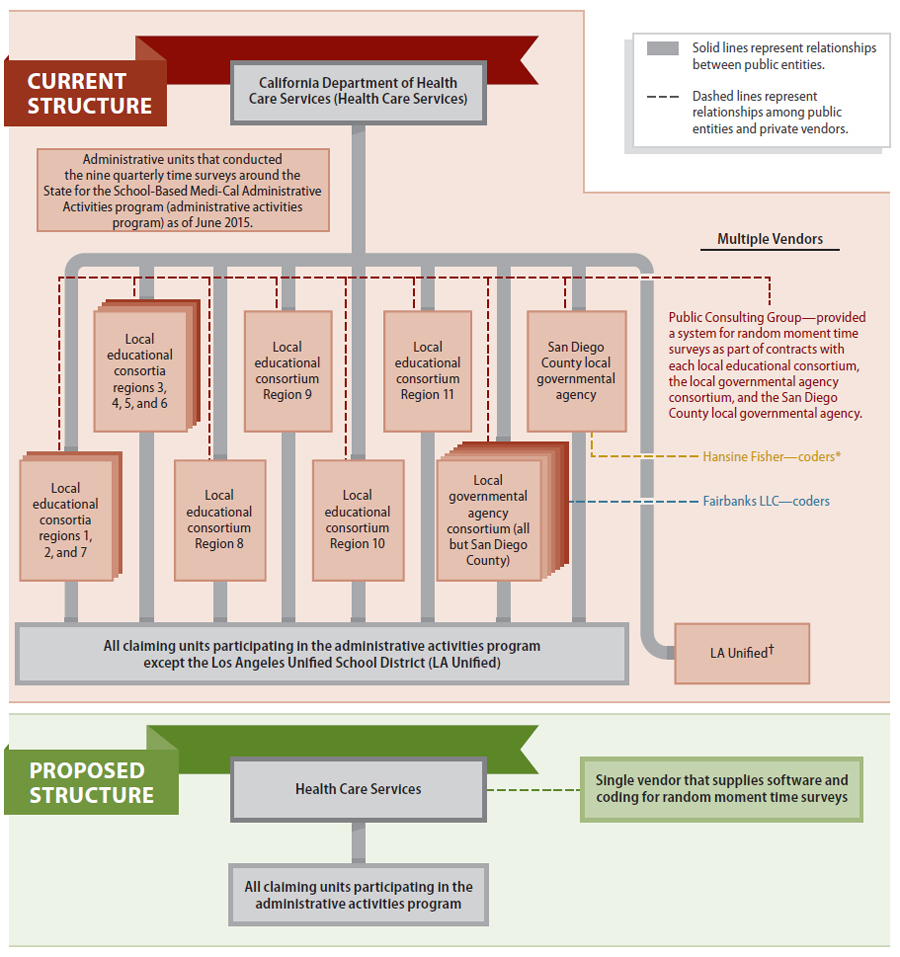
Sources: Documents obtained from staff of Health Care Services and from the websites of Health Care Services and LA Unified.
* According to Health Care Services’ documentation, all local educational consortia use their own in-house staff for coding survey responses. Local governmental agencies use vendors for coding survey responses. Coding categorizes the activity a time survey participant performed during a randomly selected moment and determines whether that activity is reimbursable by the administrative activities program.
† In October 2010 the Centers for Medicare and Medicaid Services approved LA Unified’s plan to perform its own time surveys. This district submits its reimbursement claims to Health Care Services through the Region 11 local educational consortium.
Local educational consortia and local governmental agencies implemented more than one quarterly time survey. According to the chief of Health Care Services’ School-Based Administrative Activities Unit (section chief), Health Care Services did not impose any requirements on these entities when they were forming administrative units to conduct random moment time surveys. The local educational consortia and the local governmental agencies each issued a single request for proposals to identify a vendor to help them implement the new methodology; they each selected the same vendor, but they did not each decide to conduct a single quarterly time survey. The San Diego County local governmental agency conducts its own quarterly time survey, while the remaining seven local governmental agencies formed a consortium to conduct a single quarterly time survey for their claiming units. Four local educational consortia banded together to conduct a single quarterly time survey of their claiming units while three other local educational consortia banded together to conduct a single quarterly time survey of their claiming units. The remaining four local educational consortia each conduct their own individual quarterly time surveys. As a result, the local educational consortia and local governmental agencies conduct a total of eight quarterly time surveys among them.
By conducting nine separate time surveys each quarter, when LA Unified is included, rather than a single statewide quarterly time survey, participants in the administrative activities program expend nine times the effort and incur corresponding additional costs to complete, code, and assure the quality of the time survey responses. If Health Care Services implemented a single statewide quarterly time survey, it could reduce the administrative activities program’s cost by avoiding these duplicative tasks. Although the costs and effort to set up a quarterly time survey—such as assembling and submitting roster reports and participant pools and identifying the total pool of time study moments available to survey—would be similar for one quarterly time survey as it is for nine, the costs and effort to complete, code, and assure the quality of the survey responses would decrease significantly if Health Care Services conducted that single survey. Each time survey requires a minimum number of survey responses to achieve a statistically valid result; this minimum number increases as the number of potential survey respondents increases. However, statistical calculations show that once each pool of time survey participants reaches a certain size— roughly 270 full-time employees—no additional survey responses are necessary to achieve a statistically valid estimate, no matter how many more employees are added to the pool. For instance, rather than issuing 49,698 survey moments as required under the current structure using nine administrative units, Health Care Services could conduct a single statewide quarterly survey requiring just 5,522 survey moments.
In addition, the local educational consortia or local governmental agencies must review and code each of the assigned moments to indicate whether the activity the employee reported is reimbursable by the federal government under the administrative activities program. Health Care Services requires at minimum two primary coders to review each completed survey and assign an activity code and a senior coder to ensure that the primary coders correctly coded the survey and to resolve any discrepancies. We estimate that the administrative activities program could save as much as $1.3 million annually in coding costs alone if Health Care Services conducted a single statewide quarterly time survey. These savings would be shared equally by claiming units and the federal government.
Program costs and effort would also be saved during the multi-step quality assurance process that local educational consortia, local governmental agencies, and Health Care Services must perform as described in the June 2014 California School-Based Medi-Cal Administrative Activities Manual (manual).15 Health Care Services requires local educational consortia and local governmental agencies to review a minimum of 10 percent of all coded survey responses each quarter to ensure that survey participants respond completely, that responses are properly coded, and that the senior coder or survey administrator corrects all coding errors. In addition, it requires local educational consortia and local governmental agencies to review a minimum of 10 percent of the clarifying questions that the coders asked to ensure that the coders did not ask leading questions.16 Health Care Services further requires local educational consortia and local governmental agencies to prepare summary reports of their quality assurance reviews and retain them in an audit file to be made available to Health Care Services or CMS. Finally, Health Care Services requires each local educational consortium and local governmental agency to submit its quarterly quality assurance reviews to Health Care Services. For its part, to ensure that the quality assurance process is applied statewide with consistency, Health Care Services is required to randomly select a minimum 10 percent sample of each quarter’s coded responses and clarifying questions and validate the sample. The validation process must consist of reviewing the survey responses, the assigned codes, and the clarifying questions to determine whether the code accurately reflects the activities performed, whether the activities performed were necessary for proper administration of the program, that no direct medical services were included within an administrative activity code, and that coders did not ask leading questions. Based on the extent of the activities that Health Care Services includes as part of the quality assurance process, it seems reasonable to us that the administrative activities program would save a significant amount of money and effort if local educational consortia, local governmental agencies, and Health Care Services performed quarterly quality assurance reviews on a sample of 10 percent of the responses from a single statewide quarterly time survey rather than a sample of 10 percent of the responses from eight surveys.
Other States Conduct Statewide Random Moment Time Surveys and Communicate Directly With Claiming Units
Not only would a single statewide quarterly time survey save money, but implementing that time survey would also render local educational consortia and local governmental agencies unnecessary for the administrative activities program. State law currently requires claiming units to submit administrative claims to a local educational consortium or a local governmental agency. When reviewing the organizational structure of other states’ administrative activities programs, we identified two states that have implemented a single statewide quarterly time survey since 2007. According to the U.S. Department of Education, Illinois had 1,075 school districts during the 2011–12 school year, which is comparable to California’s 1,187 school districts. Illinois transitioned its time study methodology from a worker log to a statewide random moment time survey in 2009 in order to simplify its Medicaid claiming process, reduce local educational agency staff time in completing claims, and increase the reliability of the claims.
Before implementing its single survey, Illinois had allowed school districts to compile their reimbursement claims independently or through cooperative arrangements between multiple school districts, and some individual and cooperating groups of local educational agencies entered into agreements with billing agents or consultants to assist them with the claim filing process. For example, the Peoria, Illinois consortium submitted administrative claims to the state on behalf of hundreds of school districts. According to a public service administrator at the Illinois Department of Healthcare and Family Services, the consortium was responsible for training member districts on completing their time surveys, and it received reimbursement from the state and distributed it to member districts. When the state implemented its statewide quarterly random moment time survey, this practice stopped. According to the public service administrator, Illinois operates its program now with five state agency staff. In addition, Implementing a single statewide quarterly time survey would save money and also render local educational consortia and local governmental agencies unnecessary for the administrative activities program. the program uses a vendor to help administer its quarterly surveys and code the survey responses, and it charges claiming units 4 percent of their claim amounts to help cover its costs.
Similarly, Texas replaced its worker log time study methodology with a statewide quarterly time survey in 2007. According to the U.S. Department of Education, Texas had 1,262 school districts during the 2011–12 school year. A rate analyst with the Texas Health and Human Services Commission told us that under the worker log methodology, school districts had the option to participate in the administrative claiming program as a stand-alone district or as part of a consortium. When Texas transitioned its time study methodology from a worker log to a random moment time survey, it did not include the consortium option in its administrative claiming program. The rate analyst explained that the single statewide quarterly time survey negated the need for such consortia and was more cost-effective and simpler to oversee. According to the director of cost reporting, time study, and data support services, Texas operates its program with eight state agency staff and uses a vendor to help administer its quarterly surveys and code the survey responses. Texas withholds a maximum of 5 percent of claiming units’ federal reimbursements to help cover its costs.
On the other hand, a third state we examined—Michigan— employs a structure similar to California’s for its administrative claiming program. According to the U.S. Department of Education, Michigan had 869 school districts during the 2011–12 school year. Michigan’s regional educational services agencies, known as intermediate school districts, submit reimbursement claims that include administrative costs from multiple local school districts. However, Michigan conducts a single statewide quarterly time survey to calculate the claim amounts for these agencies. Michigan charges intermediate school districts for the costs of three staff, uses a vendor to help administer its quarterly time surveys and code the survey responses, and allocates the actual costs of its program to the intermediate school districts and other education institutions proportionately based on student counts.
Health Care Services delegated implementation of the new survey methodology to the local educational consortia and the local governmental agencies and did not retain this responsibility itself because it did not believe that it had the time to acquire the necessary software. According to the assistant chief of its Safety Net Financing Division (assistant division chief), Health Care Services originally explored the possibility of developing custom software for statewide use rather than purchasing licensing software from a vendor. The assistant division chief also indicated that Health Care Services rejected this idea because it was attempting to comply with a CMS-imposed timeline for implementing the new methodology and that the length of the state procurement process did not allow Health Care Services to comply with that timeline. She added that Health Care Services delegated responsibility to procure a random moment time survey system to the local educational consortia and the local governmental agencies because it wanted claiming units to get reimbursed quickly for their deferred claims. However, CMS appears to have been flexible regarding timelines. According to one of its representatives, the role CMS had in relation to the implementation date of the new methodology was to consider Health Care Services’ proposals and to work with Health Care Services on implementing the new methodology because CMS required all administrative activities costs from July 2012 forward to be based on the new methodology. He also stated that as of February 2015, CMS has approved every extension request Health Care Services made regarding implementation of the new methodology. Regardless of the difference of opinion, now that it has begun paying deferred claims to claiming units, Health Care Services has the opportunity to reevaluate its decision to delegate responsibility for the surveys to the local educational consortia and local governmental agencies.
In addition to Texas’ use of a statewide random moment time survey and its use of a standard contract for claiming units to print, sign, and submit (mentioned in Chapter 1), we observed another practice Texas’ Medicaid agency uses that California could adopt to help to ensure the clarity and effectiveness of administrative activities program communication. Texas’ Medicaid agency posts on its website a frequently asked questions, or FAQ, document that answers questions claiming units ask during training sessions or submit to the agency by phone or email. This nine-page FAQ answers general questions—for instance, those pertaining to eligibility requirements to participate in the program—and more specific ones—such as those pertaining to training requirements and filing reimbursement claims. Texas updates the FAQ as needed; the document was last updated in January 2015. In contrast, Health Care Services has posted various FAQs to its website based on questions asked during annual administrative activities program training sessions going back to 2007. However, these documents have not been updated since 2012 and do not adequately reflect current policy and therefore would be of little value to claiming units with policy questions.
The Structure of the Administrative Activities Program May Prevent Some Claiming Units From Receiving the Full Amount of Interim Payments
The administrative activities program’s use of local educational consortia and local governmental agencies also affects Health Care Services’ ability to promptly make the full amount of interim payments to some claiming units in accordance with the settlement agreement with CMS. Because Health Care Services issues interim payments to local educational consortia and local governmental agencies and not to individual claiming units, it appears that some claiming units will not promptly receive their full interim payment amounts as described in the settlement agreement. As discussed in the Introduction, the terms of the settlement agreement authorized Health Care Services to make interim payments based on a percentage of the original amounts of the deferred reimbursement claims. These interim payments were intended to provide claiming units a portion of the funds for their deferred claims before Health Care Services fully resolved these claims, which Health Care Services estimates could be as late as 2019.
However, Health Care Services’ payments to local educational consortia and local governmental agencies were not always large enough to cover the interim payments owed to some claiming units because of previous overpayments made to other claiming units. Further, as of August 2015, it was not clear how Health Care Services would ensure that each claiming unit would receive the amount to which it is entitled under the settlement agreement. For example, the Sacramento City, Folsom Cordova, and San Juan unified school districts submitted reimbursement claims through the Sacramento County local governmental agency. Health Care Services previously paid these same claiming units for certain reimbursement claims that CMS subsequently deferred. As such, Health Care Services considered those reimbursement amounts to be overpayments. As part of the process to resolve the deferred claims, these three claiming units are entitled to receive interim payments under the terms of the settlement agreement. However, for the claims considered in June 2015, the overpayments to other claiming units within the Sacramento County local governmental agency were larger than the interim payment amount owed to the San Juan Unified School District. As a result, the district did not receive the more than $76,000 to which it was entitled under the settlement agreement.
Similarly, it appears that some claiming units in the Los Angeles County local educational consortium did not receive their full interim payments. Health Care Services paid the consortium only $55,000 to cover more than $2 million in interim payments owed to some claiming units because other claiming units within the consortium had overpayments that totaled more than their interim payments. According to the section chief, Health Care Services is working to resolve this issue. Although Health Care Services should eventually resolve all deferred claims as described in the settlement agreement, it may be as late as 2019 before this process is complete.
Recommendations
To streamline the organizational structure of the administrative activities program and to improve the program’s cost-effectiveness, the Legislature and Health Care Services should implement the following recommendations, thus allowing California to eliminate the need for local educational consortia and local governmental agencies to participate in the program.
Legislature
To streamline the organizational structure of Health Care Services’ administrative activities program and to improve the program’s cost-effectiveness, the Legislature should amend state law to allow claiming units to submit reimbursement claims directly to Health Care Services.
Health Care Services
To streamline the organizational structure of its administrative activities program and to improve the program’s cost-effectiveness, Heath Care Services should take the following actions to implement a single statewide quarterly random moment time survey:
- Develop and implement a plan to take over responsibility for conducting quarterly time surveys and performing related activities as soon as reasonably possible.
- Develop and issue a request for proposals to identify a responsible vendor to assist in implementing a statewide quarterly random moment time survey.
- Draft revisions to regulations as appropriate and to applicable documents, including the manual, oversight strategies and plans, and policy and procedure letters.
In addition to our earlier recommendation related to streamlining, Health Care Services should take the following actions:
- To the extent that local educational consortia and local governmental agencies are no longer involved in the administrative activities program, Health Care Services should develop and issue a standard contract for claiming units to sign to participate in the program.
- To improve the clarity and effectiveness of program communication, Health Care Services should develop and implement feedback mechanisms, such as organized, up-to-date FAQs, through which it can communicate results of relevant inquiries to other stakeholders, including claiming units.
- To better ensure that some claiming units do not unfairly disadvantage other claiming units in the receipt of interim payments, Health Care Services should explore opportunities to expedite consistent, timely, and fair interim payments to those claiming units with no overpayments. Health Care Services should involve representatives of local educational consortia, local governmental agencies, and claiming units in these efforts and communicate the results to interested stakeholders.
Chapter 3
OTHER SHORTCOMINGS EXIST IN THE CALIFORNIA DEPARTMENT OF HEALTH CARE SERVICES’ ADMINISTRATION OF SCHOOL-BASED MEDI-CAL PROGRAMS
Chapter Summary
The California Department of Health Care Services (Health Care Services) has displayed certain weaknesses in its administration of school-based Medi-Cal programs, which consists of the School-Based Medi-Cal Administrative Activities program (administrative activities program) and the Local Educational Agency Medi-Cal Billing Option Program (billing option program). For instance, Health Care Services has not maximized the participation of claiming units in the administrative activities program.17 We estimate that 275, or 27 percent, of the 1,004 local educational agencies did not participate in the administrative activities program during fiscal year 2011–12, resulting in a loss to the State of an estimated $10.2 million in federal reimbursements. In addition, Health Care Services delegated responsibility for maximizing claiming unit participation to local educational consortia and local governmental agencies, but it did not adequately oversee their efforts.18 Health Care Services also did not maximize federal reimbursement for the administrative activities program by failing to authorize claiming units to claim reimbursement for translation activities at a 75 percent rate as federal law currently allows rather than the 50 percent rate it previously allowed. Because the claiming units used the lower rate, we estimate that they failed to claim $4.6 million in federal funding from February 2009 through June 2015.
We also observed that as of August 2015, Health Care Services had not yet adopted required regulations despite state laws in effect for more than 15 years to do so. Health Care Services’ failure to adopt regulations for its administrative activities program limits the public’s ability to participate fully in developing the rules governing it. In addition, we believe that stakeholders could construe Health Care Services’ policies as underground regulations, which could make them unenforceable under California’s Administrative Procedure Act (APA), and thus could potentially interrupt reimbursement payments to claiming units.
Finally, Health Care Services has not filed a required annual report for the billing option program with the Legislature since February 2013. By not filing the report annually as required, Health Care Services has failed to provide the Legislature and other stakeholders with timely and relevant information, including program successes and barriers.
Health Care Services Has Not Maximized Federal Reimbursements for its Administrative Activities Program
Health Care Services has not maximized federal reimbursements applicable to the administrative activities program. For instance, we observed that even though the number of claiming units participating in the administrative activities program increased since we last identified this as a concern, Health Care Services still has not adequately maximized claiming units’ participation. In our August 2005 audit report titled Department of Health Services: Participation in the School-Based Medi-Cal Administrative Activities Program Has Increased, but School Districts Are Still Losing Millions Each Year in Federal Reimbursements (report number 2004-125), we pointed out that 679, or 65 percent, of local educational agencies were not participating, costing California $52.7 million in lost reimbursements. Based on our current examination of information from Health Care Services and the California Department of Education, we estimate that 275, or 27 percent, of the 1,004 local educational agencies still were not participating in the administrative activities program during fiscal year 2011–12.19 We estimate that these 275 claiming units missed out on claiming $10.2 million in federal reimbursements for that same fiscal year. Furthermore, based on Health Care Services’ claiming data and participant lists that local educational consortia and local governmental agencies filed, approximately 145 claiming units that filed claims in fiscal year 2011–12 did not participate in the random moment time study in the third quarter of fiscal year 2014–15, resulting in less federal funding to the State.
We believe that as the single state agency designated by state law to administer Medicaid in California, Health Care Services should ensure that claiming units participate in the administrative activities program to the greatest extent reasonably possible. One way to obtain this assurance is to conduct outreach activities to nonparticipating claiming units to encourage them to participate. The administrative activities program staff in other states—including those in Illinois and Texas—informed us that they perform outreach at the state agency level to encourage participation in their programs. For instance, the Medicaid administering agency within Texas—the Health and Human Services Commission—partners with the Texas Education Agency to distribute messages at least yearly containing outreach materials to promote the administrative activities program to all school districts in Texas.
Under the current structure of California’s administrative activities program, Health Care Services has delegated outreach responsibility to the local educational consortia and local governmental agencies. However, Health Care Services does not gather any information to assess the results of these entities’ outreach efforts, such as the number and names of nonparticipating claiming units that could participate in the administrative activities program. Health Care Services’ chief of the Medi-Cal Administrative Claiming Section (section chief) stated that Health Care Services could determine which claiming units have participated in the past and have since dropped out, but it has no way to identify those claiming units that have never participated. Additionally, the assistant division chief of the Safety Net Financing Division (assistant division chief) stated that Health Care Services will be looking for ways to bring back claiming units that have dropped out and will discuss how to expand the program to other claiming units in the future. Without knowing the total number of nonparticipating claiming units that could participate in the administrative activities program and who they are, Health Care Services cannot assess whether the local educational consortia and local governmental agencies are performing adequate outreach to nonparticipating claiming units on the department’s behalf and encouraging these units to participate in the program
Health Care Services also has not maximized the federal reimbursement amount available for one type of activity allowed in a school-based setting. For the six fiscal years from 2009–10 through 2014–15, Health Care Services allowed claiming units to claim a 50 percent federal reimbursement rate for translation services, one of the allowable activities, when the maximum reimbursement rate was actually 75 percent. Activities covered by translation include assisting a student or parent in accessing or understanding California’s Medicaid program (Medi-Cal) application process or treatments that Medi-Cal covers. Without knowing the total number of nonparticipating claiming units that could participate in the administrative activities program and who they are, Health Care Services cannot assess whether the local educational consortia and local governmental agencies are performing adequate outreach to nonparticipating claiming units.
Federal law allows claiming units to be reimbursed for a portion of the costs they incur for providing different types of administrative activities, and it specifies the reimbursement rates. Federal law generally authorizes a reimbursement of up to 50 percent of costs, but for translation services federal law authorizes reimbursement of up to 75 percent. We also observed that guidance issued by other states for their administrative activities programs, including Georgia, New Mexico, and Texas, all allowed their claiming units to claim the 75 percent reimbursement rate for translation. Health Care Services, however, has allowed California claiming units to claim only a 50 percent reimbursement rate for translation, resulting in the loss of an estimated $4.6 million in federal funding from February 2009 through June 2015. This loss caused claiming units to unnecessarily use other funding sources to cover the costs of translation services within the administrative activities program.
Health Care Services did not allow claiming units to claim the higher reimbursement rate for translation because the section chief was unaware that translation services were authorized by federal law to be reimbursed at a higher rate. However, a July 2010 CMS letter addressed to the directors of Medicaid state agencies (such as Health Care Services) expressly allows claiming units to use a 75 percent reimbursement rate for translation services under a federal law. The letter also says that states can claim the increased rate for allowable expenditures dating back to February 2009, the effective date of the federal law. However, Health Care Services took no action to increase the reimbursement rate for translation services from 50 percent to 75 percent even after telling CMS in October 2013 that it was aware of the increased rate. Once she became aware of the July 2010 CMS letter, the assistant division chief confirmed that Health Care Services found nothing to prevent the claiming of translation activities at 75 percent and that the department will contact CMS to discuss the increased rate.
Health Care Services Did Not Adopt Regulations That State Law Requires
Health Care Services’ failure to comply with state law regarding the adoption of regulations for its administrative activities program limits the public’s ability to participate fully in developing the rules governing it. Four subdivisions of Section 14132.47 of the California Welfare and Institutions Code require Health Care Services to adopt regulations for the administrative activities program. For example, one of these subdivisions requires Health Care Services to consult with local educational consortia and local governmental agencies to adopt regulations regarding the submission and payment of administrative activities claims and to deny any claim from a participating local educational consortium or a local governmental agency if it determines that the claim is not supported in accordance with criteria established pursuant to this law and implementing regulations.
Although these statutory requirements have been in effect for more than 15 years, as of August 2015, Health Care Services had not yet adopted the regulations as called for. According to the section chief, Health Care Services did not adopt these regulations because it believed that its manual and policy and procedure letters provided the necessary guidance to stakeholders. We observed that the 2014 edition of this manual is a 151-page document consisting of 11 sections and eight appendices, collectively governing how program participants are to develop, submit, process, and receive reimbursement claims. For instance, to receive reimbursement, claiming units must limit flat-fee vendor reimbursements to 15 percent of the total amount claimed during a given fiscal year and must not include direct costs related to teachers. If claiming units fail to comply with these requirements, their local educational consortium, local governmental agency, or Health Care Services can reject their claims. Policy and procedure letters serve to update or augment the manual with specific policies, and they impose similar requirements on program participants. Over the years, Health Care Services has issued a number of policy and procedure letters related to the administrative activities program, covering topics such as establishing an appeals process and issuing a policy governing the use of electronic signatures.
Nevertheless, by not adopting regulations, Health Care Services limits the opportunities available to claiming units and to the public to participate in the regulatory process. The APA defines a regulation as any rule of general application adopted by any state agency to implement, interpret, or make specific the law enforced or administered by it, or to govern its procedure. The APA requires state agencies to submit proposed regulations through a process that allows public comment and review by the Office of Administrative Law (office). According to the office, which administers the APA, the State designed the requirements of the APA to provide the public with a meaningful opportunity to participate in the adoption of state regulations and to ensure that regulations are clear, necessary, and legally valid. One way the APA provides meaningful opportunities to participate in the adoption of regulations is the minimum 45-day public comment period. After an agency publishes and issues the notice of proposed rulemaking, the public has the opportunity to submit written, faxed, or emailed comments to the agency regarding the proposed rules; the public may participate in any public hearing on the proposal; and the public may review the adopting agency’s written summary of its responses to the submitted comments.
As a result, not developing regulations means claiming units, which have demonstrated in the past their willingness to identify concerns when Health Care Services implemented changes to the administrative activities program, may not have their voices heard. For instance, when it implemented the random moment time survey methodology discussed in Chapter 2, claiming units voiced concerns, including that Health Care Services’ manual and website were incomplete and that Health Care Services provided inaccurate and inadequate training. While Health Care Services does hold stakeholder meetings, state law does not require written responses to questions that local educational agencies raise during those meetings, unlike what the APA would require in the adoption of regulations.
Furthermore, if a state agency issues a requirement that meets the definition of the term regulation without following the APA when it is required to do so, this requirement is called an underground regulation. State law allows anyone to file a petition with the office to determine whether a state agency’s policies containing such requirments are underground regulations. The office also stated that state agencies are prohibited from enforcing underground regulations. Because Health Care Services issued policies rather than adopting regulations that local educational consortia, local governmental agencies, and claiming units must follow as part of the administrative activities program, we believe that stakeholders—including any member of the public—could construe the manual and the policy and procedure letters as underground regulations. By using and enforcing its manual and its policy and procedure letters rather than adopting them as regulations in accordance with the APA, Health Care Services may also risk interrupting the flow of federal reimbursement funds to claiming units. If someone were to successfully challenge the manual and the policy and procedure letters as underground regulations, Health Care Services, the local educational consortia, and the local governmental agencies might be unable to use or enforce the claim reimbursement provisions included in them. The inability to use or enforce these provisions could increase the risk of an interruption to future reimbursement payments to claiming units.
Finally, although state law exempts certain policies from the APA’s requirements, we do not believe Health Care Services should seek such statutory exemptions for the administrative activities program. For instance, Health Care Services may implement state law related to Medi-Cal’s electronic medical records through provider bulletins or similar instructions without taking regulatory action; however, exempting Health Care Services from complying with the APA’s provisions related to the administrative activities program could impede the ability of claiming units to participate to the extent envisioned under the APA when Health Care Services develops administrative activities requirements with which they must comply. As we previously discussed, the APA allows all claiming units to participate in the regulatory process if they wish. We believe denying claiming units this opportunity increases the likelihood of misinterpretations and inconsistent application of administrative activities program requirements.
Health Care Services’ Lack of Required Annual Reports Limits the Transparency of the Billing Option Program
Although its most recently submitted version of an annual report for the billing option program contained all elements the law requires, Health Care Services last filed a report that was due in 2012 with the Legislature in February 2013—and has not filed another since then. State law requires Health Care Services to file an annual report with the Legislature about the billing option program. Table 5 on the following page shows the 11 elements that state law requires Health Care Services to include as part of that report. For the 2012 report covering the 14 months from April 2011 through May 2012, which is the most recent report that it filed, Health Care Services included all 11 required elements. For instance, the report identified Medicaid reimbursement revenues for California and other states for two fiscal years and discussed program successes, including increases in federal reimbursements. Health Care Services mentions that Medi-Cal reimbursements for the billing option program more than doubled from $63.6 million in fiscal year 2005–06 to $130.4 million in fiscal year 2009–10.
According to Health Care Services, this increase is due in part to its efforts to allow local educational agencies to correct previous errors in claims that caused them to be incorrectly paid or denied as well as increased federal funding due to the federal American Recovery and Reinvestment Act of 2009 (recovery act). In addition to these factors, adding more services increases the Medi-Cal reimbursement. According to the assistant division chief, Health Care Services reviews new guidance issued by CMS and any changes to California’s Welfare and Institutions Code for additional services that could be claimed under the billing option program. She also stated that Health Care Services identifies new services for reimbursement through a process that stakeholders initiate. The assistant division chief told us that stakeholders first notify Health Care Services of medical services they believe should be reimbursable. Next, Health Care Services begins a vetting process through which it examines other states to determine if the service is reimbursed elsewhere in the country, identifies a reasonable reimbursement rate for the service, and assesses how prevalent the need is for the particular service. Health Care Services then submits a state plan amendment, if needed, to CMS for approval to add the new service into the allowed reimbursable services. Some changes merely represent a new delivery method of currently approved services and thus do not require a state plan amendment.
Table 5
Annual Report Elements Required by the State for the Local Educational Agency Medi-Cal Billing Option Program
| 1 | An annual comparison of school-based Medicaid systems in other states. |
| 2 | A state-by-state comparison of school-based Medicaid total and per eligible child claims as well as federal revenues for the most recent two years for which data are available. |
| 3 | A summary of the California Department of Health Care Services’ (Health Care Services) activities that contributed toward narrowing the gap between California’s federal fund recovery per eligible student and that of the top three states in the report. |
| 4 | An explanation of how each activity in item (3) contributed toward narrowing the gap between California’s federal fund recovery per eligible student and that of the top three states in the report. |
| 5 | A listing of all school-based services, activities, and providers approved for reimbursement by the Centers for Medicare and Medicaid Services (CMS) in other state plans that are not yet approved for reimbursement in California’s state plan. |
| 6 | The service unit rates for all services, activities, and providers identified in item (5). |
| 7 | The official recommendations made to Health Care Services by the California Department of Education; representatives of urban, rural, large, and small school districts; county offices of education; the local educational consortia; local educational agencies; staff from Region IX of CMS; experts from the fields of both health and education; and state legislative staff. |
| 8 | The actions taken by Health Care Services for each recommendation identified in item (7). |
| 9 | A one-year timetable for state plan amendments and other actions necessary to obtain reimbursement for those items listed in item (5). |
| 10 | Identification of any barriers to local educational agency reimbursement, including those specified by the entities in item (7), that federal requirements have not imposed. |
| 11 | A description of the actions that have been and will be taken to remove the barriers identified in item (10). |
Source: Section 14115.8(f) of the California Welfare and Institutions Code.
We found that Health Care Services received higher reimbursements for the billing option program because of temporary rate increases the recovery act allowed. The recovery act increased the federal reimbursement percentages for Medicaid services from 50 percent to as much as 61.6 percent from October 2008 through June 2011.20 See the text box for the recovery act’s increased reimbursement rates and the periods to which they applied. Health Care Services passed on to the local educational agencies the higher reimbursements that occurred under the recovery act.
Medicaid Reimbursement Rates Under the American Recovery and Reinvestment Act of 2009
The American Recovery and Reinvestment Act of 2009 increased the federal reimbursement rates for the Local Educational Agency Medi-Cal Billing Option Program from 50 percent to the following percentages from October 2008 through June 2011:
From October 1, 2008, through December 31, 2010: 61.59%
From January 1, 2011, through March 31, 2011: 58.77%
From April 1, 2011, through June 30, 2011: 56.88%
Sources: American Recovery and Reinvestment Act of 2009, the Federal Register, and a California Department of Health Care Services’ Policy and Procedure Letter (PPL 11-001).
Although its most recently issued report contains the 11 required elements and describes its successes and barriers related to the billing option program, Health Care Services has not filed an annual report since February 2013, about two and a half years ago. Based on past practice, the two annual reports expected in 2013 and 2014 would have covered the roughly two-year period from April 2012 through May 2014. By not filing the required billing option program reports annually, Health Care Services unnecessarily restricts transparency by depriving the Legislature, the general public, and other stakeholders of the billing option program prompt access to program information. For example, in the report covering April 2011 through May 2012, Health Care Services mentions setting up a meeting with CMS in 2012 to discuss adding new services. However, Health Care Services presented this plan about two and a half years ago and it has still not filed a new report to disclose what, if any, progress has occurred related to these new services.
The section chief attributed the delay in issuing the report covering April 2012 through May 2013 to turnover among the executive staff that review the report and slow responses from other states for the portion of the report that requires comparisons to other states’ Medicaid agencies. The chief of Health Care Services’ Safety Net Financing Division told us in June 2015 that Health Care Services plans to release shortly the report covering the 14 months from April 2012 through May 2013, and then it will issue a single report covering the two years from April 2013 through May 2015 by December 2015. As of August 2015 Health Care Services had not yet posted the report covering the period through May 2013 to its website.
Although Health Care Services has not recently issued its required annual report for the billing option program, such a report presents information useful to stakeholders. We believe that providing similar information for the administrative activities program would also be useful. The statutory requirement for the annual report compels Health Care Services to examine routinely its billing option program for ways to improve the program and to file periodically the results of its examination in a report to the Legislature. The legislative report provides a retrospective look at program successes and barriers, and it identifies anticipated future issues and ways to address them. Writing a periodic report that the public can access forces Health Care Services to document and describe those areas where the program requires improvement. The annual requirement, when followed, provides the Legislature and stakeholders with timely access to information on potential program problems or upcoming changes. Health Care Services indicated that it does not prepare a similar annual report for the administrative activities program because the law does not presently require it to do so.
Recommendations
Legislature
To help improve and maximize the benefits of the administrative activities program, as well as to provide enhanced transparency to stakeholders, the Legislature should enact legislation as soon as possible that requires Health Care Services to prepare a report annually for the administrative activities program similar to the annual report state law requires for the billing option program.
Health Care Services
To better maximize federal reimbursements for the administrative activities program, Health Care Services should complete the following actions within six months:
- Develop and implement a method to oversee and track the outreach efforts that local educational consortia and local governmental agencies use for ensuring that nonparticipating claiming units understand the benefits and consider participating in the administrative activities program.
- Revise reimbursement rates to authorize claiming units to claim the 75 percent reimbursement rate for translation activities as federal law allows.
- Determine the extent to which claiming units can claim the unreimbursed difference between the 50 percent and 75 percent reimbursement rates for translation activities for past years and inform claiming units of the findings.
Should the Legislature implement our recommendation in Chapter 2 to allow claiming units to submit reimbursement claims directly to it, Health Care Services should develop and implement its own outreach functions to ensure that claiming units that do not currently participate understand the benefits and consider participating in the administrative activities program.
To provide the public with the ability to participate fully in developing the rules governing the administrative activities program, Health Care Services should, in accordance with the APA, immediately develop and adopt the regulations cited in the four subdivisions of Section 14132.47 of the California Welfare and Institutions Code.
To ensure that it provides stakeholders with timely access to information regarding the billing option program, Health Care Services should do the following:
- Issue the required annual report covering April 2012 to May 2013 immediately.
- Issue the required annual report covering April 2013 to May 2015 by December 2015 as promised.
- Issue all future annual reports in a timely manner.
We conducted this audit under the authority vested in the California State Auditor by Section 8543 et seq. of the California Government Code and according to generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives specified in the Scope and Methodology section of the report. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Respectfully submitted,
ELAINE M. HOWLE, CPA
State Auditor
Date: August 20, 2015
Staff:
Michael Tilden, CPA, Audit Principal
Dale A. Carlson, MPA, CGFM
Nate Jones, CFE
Ryan J. Mooney
Jesse R. Walden
Legal Counsel:
Scott A. Baxter, Sr. Staff Counsel
For questions regarding the contents of this report, please contact Margarita Fernández, Chief of Public Affairs, at 916.445.0255.
Footnotes
8According to CMS, a claiming unit is typically a school district or a program within a district. California has claiming units that are as diverse as county offices of education, special education local plan areas, local school districts, community colleges, and Healthy Start programs.Go back to text
9A local educational consortium is one of the 11 service regions of the California County Superintendents Educational Services Association. Each consortium is led by a county education office within the region. A local governmental agency is an agency of either a county or a chartered city or is a Native American Indian tribe, tribal organization, or subgroup of a Native American Indian tribe or tribal organization.Go back to text
10The school-based administrative claiming guide refers to CMS’s 2003 Medicaid School-Based Administrative Claiming Guide (guide). The purpose of the guide is to inform schools, state Medicaid agencies, and other interested parties on the appropriate methods for claiming federal reimbursement for the costs of Medicaid administrative activities performed in the school setting.Go back to text
11According to a school-based services auditor in Michigan, intermediate school districts are regional educational services agencies that help local school districts with programs and services that are best done regionally. They provide state-mandated functions like pupil accounting and special education monitoring and compliance.Go back to text
12A local educational consortium is one of the 11 service regions of the California County Superintendent Educational Services Association. Each consortium is led by a county education office within the region.Go back to text
13A local governmental agency is an agency of either a county or a chartered city, or a Native American Indian tribe, tribal organization, or subgroup of a Native American Indian tribe or tribal organization.Go back to text
14According to the federal Centers for Medicare and Medicaid Services (CMS), a claiming unit is typically a school district or a program within a district. California has claiming units that are as diverse as county offices of education, special education local plan areas, local school districts, community colleges, and Healthy Start programs.Go back to text
15The implementation plan for LA Unified’s random moment time survey describes a different quality assurance process than the one mentioned in the manual. Therefore, the calculations described in this paragraph exclude LA Unified.Go back to text
16A leading question is one that is phrased in such a manner as to suggest a desired answer.Go back to text
17According to the federal Centers for Medicare and Medicaid Services (CMS), a claiming unit is typically a school district or a program within a district. California has claiming units that are as diverse as county offices of education, special education local plan areas, local school districts, community colleges, and Healthy Start programs.Go back to text
18A local educational consortium is one of the 11 service regions of the California County Superintendents Educational Services Association. Each consortium is led by a county education office within the region. A local governmental agency is an agency of either a county or chartered city, or a Native American Indian tribe, tribal organization, or subgroup of a Native American Indian tribe or tribal organization.Go back to text
19We selected fiscal year 2011–12 to calculate our estimate because it was the latest complete year outside the two-year window that CMS gives Health Care Services to submit reimbursement claims.Go back to text
20The recovery act provided increased reimbursement rates for the billing option program; it did not provide increased reimbursement rates for the administrative activities program.Go back to text