
Use the links below to skip to the section you wish to view:
- The State Has Not Adequately Addressed Ongoing Deficiencies
Related to the Quality of Care That Nursing Facilities Provide - The Net Incomes and Use of Related Parties Rose Over the
Past Decade for the Three Companies We Reviewed - State Agencies Have Not Always Coordinated Their Oversight Efforts
or Ensured the Accuracy and Usefulness of Publicly Available Data - Other Areas We Reviewed
- Scope and Methodology
The State Has Not Adequately Addressed Ongoing Deficiencies Related to the Quality of Care That Nursing Facilities Provide
Key Points:
- Despite ongoing concerns regarding patient health and safety, serious deficiencies associated with substandard quality of care at California's nursing facilities increased from 2006 through 2015.
- Public Health has not fulfilled one of its key oversight responsibilities—to ensure that nursing facilities meet quality-of-care standards. For example, it has not conducted all of its required inspections, which are important because they verify whether nursing facilities are providing quality care in accordance with state requirements.
- Despite the fact that the Legislature intended that the State's quality assurance fee for nursing facilities be used to incentivize quality-of-care improvements, the State currently does not use it for this purpose.
The Quality-of-Care Indicators We Reviewed
Federal F–L deficiencies: This group of deficiencies indicates that Public Health identified that a nursing facility failed to comply with federal requirements, resulting either in a widespread potential for more than minimal harm or in actual harm to patient health and safety.
Federal J–L deficiencies: This group of deficiencies indicates that Public Health identified that a nursing facility failed to comply with federal requirements, causing or likely to cause serious injury, harm, impairment, or death to a resident and warranting immediate corrective action.
State AA, A, and B citations: Public Health issues AA citations when a nursing facility's violation both meets the criteria for an A citation and results in the death of a patient. Public Health issues A citations for conditions, practices, or operations that present an imminent danger or a substantial probability of death or serious harm. B citations encompass a broad range of violation types, including emotional, financial, or actual harm to a patient; violations of patients' rights; a facility's failure to report abuse; or failure to post required public information.
Source: California State Auditor's analysis of federal and state law and the CMS State Operations Manual.
Note: We acknowledge there are many quality‑of‑care indicators; however, we focused our review on the above indicators because Public Health uses these indicators to evaluate nursing facility performance and to enforce compliance with state or federal law.
Significant Deficiencies Related to the Quality of Care That California's Nursing Facilities Provide Have Persisted for More Than a Decade
In 2007 the Legislature declared that California's public policy is to ensure that nursing facilities provide the highest level of care possible; however, our analysis shows that over the last decade, Public Health has issued an increasing number of serious deficiencies related to substandard quality of care, which we describe in the text box. We analyzed federal deficiencies and state citations because Public Health uses this information to evaluate nursing facility performance and to enforce compliance with state or federal law.4 When Public Health performs an inspection and identifies that a nursing facility has violated any state or federal law or regulation, it must issue a notice to correct the violation. Public Health issues F–L deficiencies for such federal violations as infection outbreaks, neglect, and abuse, while J–L deficiencies represent the most serious violations. Public Health can also issue state deficiencies for violations of state law; however, we focused our review on federal deficiencies. After Public Health issues a federal deficiency, it can also choose to issue a state citation if it determines the federal deficiency warrants a state citation.
We found that from 2006 through 2015, the number of both F–L and J–L deficiencies that Public Health identified increased, as shown in Table 2. Over the same period, the number of nursing facility beds industrywide did not change significantly, and this fact eliminates a potential cause for the increase in deficiencies. We are particularly concerned with the 35 percent increase in J–L deficiencies, which Public Health refers to as immediate jeopardies. These deficiencies represent facility noncompliance that did or could have resulted in serious injury, harm, or impairment to patients, including death. For each year from 2006 through 2015, Public Health issued between 28 and 94 J–L deficiencies, with the total number of J–L deficiencies exceeding 500 for this period.
| NUMBERS OF DEFICIENCIES OR CITATIONS INDUSTRYWIDE |
|||
|---|---|---|---|
| QUALITY-OF-CARE INDICATOR | 2006 | 2015 | PERCENTAGE CHANGE FROM 2006 THROUGH 2015 |
| Federal F–L deficiencies | 445 | 585 | ↑ 31% INCREASE |
| Federal J–L deficiencies | 46 | 62 | ↑ 35% INCREASE |
| State citations | 459 | 302 | ↓ 34% DECREASE |
Source: California State Auditor's analysis of Public Health's deficiency and citation data.
Note: The numbers of deficiencies and citations represent Public Health's identifications of federal requirement violations. Public Health identifies F–L deficiencies for such situations as infection outbreaks, patient neglect, and patient abuse, with J–L deficiencies indicating the most concerning violations. We limited citation data to AA, A, and B citations—generally associated with harm to nursing home patients—because these citations correspond to the most egregious violations. Interestingly, from 2006 through 2015, the total number of nursing facility beds in California did not change significantly, so variations in numbers of beds could not have caused the notable fluctuations in the numbers of deficiencies and citations industrywide.
We are also concerned that while the number of federal deficiencies Public Health identified increased, the total number of state citations it issued decreased.5 After it identifies a federal deficiency, Public Health determines whether that deficiency warrants a state citation in addition to a recommendation for a federal enforcement remedy, such as denial of Medi-Cal and Medicare payments or a requirement for additional training. A citation requires the nursing facility to pay a state penalty. The monetary penalties associated with citations increase in amount based on the severity of the violations. Citations can serve as additional deterrents to ensure that nursing facilities do not allow the same violations to recur in the future.
Nonetheless, according to Public Health's data, it issued citations for only 15 percent of its inspections that found J–L deficiencies—the most serious deficiencies—from 2006 through 2015. Moreover, Public Health also significantly reduced the number of citations it issued from 2006 through 2015, as Figure 6 shows. When we asked Public Health why it did not issue more citations for J–L deficiencies, the chief of field operations for long-term care stated that although the criteria for federal J–L deficiencies and state citations align, the burden of proof required for state citations is higher than for federal J–L deficiencies. She also acknowledged that Public Health has not recently analyzed citation issuance to assess trends in state enforcement or causes associated with those trends. Overall, we are concerned that when Public Health does not issue citations for J–L deficiencies and penalize nursing facilities for their failures, Public Health decreases its effectiveness in ensuring that nursing facilities provide quality patient care.
Figure 6
From 2006 Through 2015, Public Health Significantly Reduced the Number of AA, A, and B Citations It Issued to Nursing Facilities

Source: California State Auditor's analysis of Public Health's citations data.
Quality-of-care trends may also be attributable to Public Health's increasing its enforcement by issuing more federal deficiencies. Specifically, according to the assistant deputy director of Public Health's Center for Health Care Quality, the increase in federal deficiencies and decrease in state citations is more a measure of changes to Public Health's oversight and not necessarily an indicator of changes to the quality of care in the industry. He went on to state that Public Health issues fewer state citations because it believes that federal deficiencies have more immediate consequences for nursing facilities and can result in higher penalty amounts. Regardless, state law gives Public Health the ability to issue state citations for federal deficiencies, and, in a July 2010 letter, it informed nursing facilities that it would consider doing so for all F–L and J–L deficiencies it identified.
When we analyzed the three quality-of-care indicators described in the text box on page 13 for the three companies we reviewed, we found that Plum and Longwood compare favorably to the rest of the industry in California and that Brius received more federal deficiencies and state citations compared to the rest of the industry. In Table 3 we summarize the performance of the three companies and the industry as a whole by each indicator depicted as an average over a 10-year period. In a separate analysis, we found that the number of F–L and J–L deficiencies per 100 beds increased for all three companies since 2006, whereas the number of citations per 100 beds decreased for Plum and Longwood but increased for Brius. When we shared these results with Brius, the owner stated that he believes the vast majority of facilities he purchases are distressed facilities that, without intervention, would be forced to close due to financial or regulatory problems. He went on to state that this business model leads to a higher number of deficiencies due to the condition of the facilities and the significant time it takes to turn them around. Nonetheless, even if some of this increase in deficiencies is attributable to Public Health's increasing its enforcement efforts or due to the condition of facilities upon purchase, these deficiencies still represent instances in which Public Health identified substandard quality of care.
We also analyzed California's performance on other nationally tracked quality-of-care indicators and found that although the State performed well for certain indicators, room for improvement exists. Specifically, we assessed California's performance on several indicators CMS tracks nationally, including some that CMS uses to develop its five-star quality rating system—a resource CMS established to help consumers, their families, and caregivers compare nursing homes more easily. We found that according to CMS data from February 2018, California ranked in the top 10 best states for such indicators as total nurse staffing hours per patient per day. Compared to most other states, California also had a lower percentage of short-term residents with pressure ulcers and a lower percentage of long-term residents who fall and experience major injuries. However, California was below the national average on such indicators as the percentage of residents who were physically restrained and the percentage of short-term residents who were successfully discharged into the community. Additionally, 22 percent or 260 of California's nursing homes received either one- or two-star ratings from CMS in February 2018. A two‑star rating indicates that a nursing home is below average and a one‑star rating indicates that a nursing home is much below average. Part of the reason that California nursing homes have low ratings is the high number of deficiencies they receive.
| QUALITY-OF-CARE INDICATOR | BRIUS | PLUM | LONGWOOD | ALL FACILITIES IN THE INDUSTRY |
|---|---|---|---|---|
| Federal F–L deficiencies per 100 beds | .60 | .33 | .30 | .46 |
| Federal J–L deficiencies per 100 beds | .13 | .04 | .02 | .05 |
| State citations per 100 beds | .52 | .35 | .29 | .41 |
Source: California State Auditor's analysis of cost report data and Public Health's deficiency and citation data.
Note: Using each facility's final cost report for each year, we calculated the number of patient beds for each company. A smaller number indicates a better score.
Public Health Has Not Taken Adequate Action to Increase the Quality of Care That Nursing Facilities Provide
Public Health's actions are inadequate to ensure that nursing facilities provide improved quality of care. The mission for Public Health's Center for Health Care Quality is to protect patient safety and ensure quality care for all patients in health facilities, including nursing facilities. It also supports CMS by ensuring federal recertification of nursing facilities for participation in Medi-Cal and Medicare. However, the Center for Health Care Quality has not adequately fulfilled all of its oversight responsibilities related to approving nursing facility licensure applications, ensuring that Public Health's district offices periodically inspect nursing facilities, and issuing citations and penalties. Our review of Public Health's oversight demonstrated the need for Public Health to improve its performance in each of these areas.
Because of Its Poorly Defined Review Process and Inadequate Documentation, Public Health's Licensing Decisions Appear Inconsistent
Public Health's licensing decisions appear inconsistent because of its poorly defined review process and inadequate documentation. When Public Health receives an application for a company that wants to operate additional nursing facilities, it must perform a comprehensive review of the applicant—the company and the individuals involved in the company's management—to determine whether it has historically operated facilities in compliance with federal and state requirements. To assist Public Health in its determination of compliance, which contributes to its decision to approve or deny an application, analysts develop compliance histories that document all of the federal F–L deficiencies, state citations, and substantiated complaints an applicant's facilities have received. However, we found that the compliance histories the analysts generated are often incomplete and that the reviews performed by Public Health sometimes appear inconsistent because its process did not clarify an applicants' ability to comply with federal and state requirements. Public Health also has not adequately documented the factors it used or how it used them when making decisions to approve or deny applications, and this inadequate documentation made it difficult for us to understand Public Health's decisions. We summarize the licensing review process and our concerns with the review process in Table 4.
We analyzed Public Health's licensing review process from 2013 through 2015 for 10 applications submitted by the three companies we reviewed. Specifically, we reviewed five Brius applications, three Longwood applications, and two Plum applications. For nine of the applications, the companies submitted additional applications seeking approval to manage between one and four additional facilities at the same time as the applications we reviewed. For the remaining application we reviewed, Brius sought approval to manage 18 additional nursing facilities that Brius's owner acquired from bankruptcy; the applications associated with these facilities are currently pending. When the companies submitted to Public Health the applications we reviewed, they already owned and operated many facilities. Ultimately, Public Health approved the applications for Longwood and Plum, but it approved only one of the Brius applications we reviewed. Public Health denied three of the Brius applications, and one application is currently pending.
However, based on the documentation available in Public Health's files, it is difficult for us to understand its decisions to approve or deny some of the applications we reviewed. For example, for one of the two Plum applications, Public Health's compliance histories contain no information about the owners of Plum. According to the chief of field operations for long-term care, Public Health believes an analyst produced and reviewed a compliance history but did not print the compliance history and include it in the file for this application. Using the information that was available in the file and additional information subsequently provided by Public Health, we were unable to confirm whether it assessed Plum's compliance history before approving Plum's application to operate two additional facilities.
| PUBLIC HEALTH'S LICENSING PROCESS | CONCERNS ABOUT THE PROCESS | SCORECARD |
|---|---|---|
| Public Health reviews the applications it receives for completeness, accuracy, clarity, and consistency. | Public Health's analysts generally documented their reviews of the 10 licensing applications we assessed. | ✓ |
| An analyst creates compliance histories for all facilities associated with the company that applies to operate a nursing facility and develops compliance histories for the applicant's owners, board of directors, partners, managers, and members. | Nine of the 10 compliance histories we assessed were incomplete because Public Health did not document that it reviewed the compliance histories for the applicants, or for their owners, board of directors, partners, managers, or members. | X |
| To complete the compliance history, the analyst counts the number of federal deficiencies, state citations, and substantiated complaints issued to each of the applicant's related facilities for the three preceding years. | Although the analyst compiles these data, the analyst does not develop an overall score or rating to guide Public Health's decision making. | X |
| The analyst assesses whether the applicant demonstrated its ability to comply with Public Health's rules and regulations. | Public Health has not specified the application elements that would demonstrate a company's ability to comply. | X |
| An analyst and the unit manager approve the application or submit it for additional review by higher-level management, such as the deputy director of licensing and certification. | There is no objective threshold indicating when an analyst, the unit manager, or both should elevate reviews to higher‑level management. | X |
| If higher-level management reviews the application, they can consider any additional factors that are relevant, such as CMS five-star ratings, the applicant's size and growth pattern, the applicant's noncompliance with laws overseen by other agencies like Health Care Services, and federal or state enforcement actions, such as penalties or the withholding of Medi-Cal payments. | Public Health has not defined or documented in policy, procedures, or regulations the additional factors its higher‑level management may consider or how it may use them in making licensing decisions. Although higher-level management stated that their approval and denial decisions were sometimes based on these factors, the use of these factors is not adequately documented. | X |
Sources: California State Auditor's analyses of state law; Public Health's compliance history procedures; compliance history files for 10 licensing applications associated with Brius, Plum, and Longwood from 2013 through 2015; Public Health denial letters; and discussions with Public Health analysts and higher-level management.
✓ = We had minimal concerns about this part of the process.
X = We had significant concerns about this part of the process.
Moreover, it was difficult for us to determine the factors Public Health used to make its licensing decisions because its files do not specify or include documentation concerning all of the factors it considered. These omissions are especially important because the files we reviewed indicate that some applicants had relatively similar compliance histories in terms of federal F–L deficiencies and number of state citations, based on the data Public Health analysts collected at the time of their review, but received different licensing decisions from Public Health. For example, when it applied to operate one additional facility in 2014, Brius appeared to have performance similar to that of Longwood, which applied to operate one additional facility during that same year, and of Plum, which applied to operate two facilities in September 2015. According to the documentation in their application files, these companies demonstrated similar performance for two indicators: the percentage of facilities owned by the applicants that had F–L deficiencies or state citations.
When we asked Public Health why it approved the Longwood and Plum applications and denied Brius's even though Public Health's documentation indicates that the applicants appeared to have similar performance on the above indicators, Public Health stated that management bases its licensing decisions not only on an applicant's compliance history but also on a broad range of other factors. We include some of these factors in Table 4. However, because Public Health did not adequately document its use of these factors in the 10 cases we reviewed, it is not apparent whether and to what extent these factors may have affected its final decisions. Therefore, although Public Health asserted that its final decision related to the Brius application was justified because of such additional factors as enforcement actions that Health Care Services had taken against Brius, we could not reach the same conclusion using the documents available in the file. Without adequate documentation, Public Health risks exposing itself unnecessarily to litigation from nursing facility applicants.
We believe that Public Health should develop a defined review process in which it reviews the same components for each applicant and applies minimum standards that would be appropriate for that class of facility.6 For example, Public Health could set thresholds for the number and severity of deficiencies and citations that would require an analyst to flag an application for additional review by higher-level management, who would then be responsible for reviewing the compliance history developed by the analyst. Higher‑level management would also be able to determine whether any additional factors, such as those described in Table 4, support an approval or denial of the application. After Public Health's management apply their professional judgment to determine whether to approve or deny a licensing application, they would then need to ensure that they adequately document their justification for that decision.
When we shared these findings with Public Health, it acknowledged the lack of adequate documentation and agreed it needed to make improvements to the licensing review process. Although Public Health also agreed that it needs to set an objective threshold that would elevate potentially concerning applications to higher‑level management for review, it expressed concerns about how to develop this threshold. Moreover, it was also concerned about our recommendation that it document all of the factors it might consider when reviewing an application. However, as a regulatory agency, Public Health needs to be transparent about its decision making. Moreover, we believe that Public Health, through collaboration with stakeholders, is capable of developing a complete list of factors and that it should work with the Legislature to codify this review process including the factors it will consider. Legislative action will be the most efficient and effective way for Public Health and stakeholders to agree on how it should assess companies seeking to operate additional nursing facilities in the future.
Public Health Has Failed to Perform Relicensing Inspections, as State Law Requires
Public Health has prioritized conducting federal recertification inspections over performing required state relicensing inspections, which ensure that nursing facilities comply with state laws. Public Health has consistently conducted federal recertification inspections, which are necessary for nursing facilities to continue their participation in Medicare and Medi-Cal. However, according to one of the Center for Health Care Quality's chiefs of field operations, Public Health has not consistently performed state relicensing inspections that are required no less than once every two years. For example, we found that Public Health had not performed in a timely manner the state relicensing inspections for three of the six facilities we reviewed. Additionally, since 2015 Public Health has failed to perform relicensing inspections for most nursing facilities in Los Angeles County, which is home to roughly 32 percent of the State's total nursing facilities. Specifically, Public Health contracted with Los Angeles County in 2015 to perform health facility oversight, but it failed to include relicensing inspections in the agreement.
State relicensing inspections are important because they ensure that nursing facilities are providing quality care in accordance with state law and regulatory requirements. Federal recertification inspections do not address some state requirements, and, in some cases, federal requirements are less stringent than state requirements. For example, state law establishes patient admission requirements for nursing facilities and prohibits nursing facilities from retaliating against patients or employees if they file complaints related to care, services, or conditions at the facilities. Furthermore, state law sets forth additional nursing training requirements. Because federal inspections do not ensure that facilities are meeting these requirements, nursing facilities' noncompliance with state requirements likely remains unchecked when Public Health fails to perform relicensing inspections.
Part of the challenge Public Health faces is that state and federal timelines for certification and licensure inspections are not aligned. A federal recertification inspection of a nursing facility must occur no later than 15 months since the last federal inspection, while state law requires Public Health to conduct its state relicensing inspection no less than once every 24 months. Effective in 2007, the Legislature authorized Public Health to conduct dual-purpose inspections that assess both federal and state requirements. According to the chief of field operations for long-term care, Public Health strives to conduct all certification and licensure inspections concurrently, but the misalignment of federal and state timelines prevents Public Health from achieving this goal. In fact, when we looked at the number of state relicensing inspections performed statewide in 2015 and 2016, we found that Public Health performed only 464 of the approximately 1,100 relicensing inspections that should have taken place during that time. If the Legislature required state relicensing inspections every 30 months, thus aligning state timelines with federal timelines, Public Health would be able to schedule its relicensing inspections more efficiently.
Public Health Has Not Ensured That It Issues Citations in a Timely Manner and That Its Penalty Amounts Present Adequate Financial Disincentives
Not only has the number of Public Health citations declined—as discussed on page 15—but Public Health has also struggled to issue citations in a timely manner. State law requires that if Public Health determines a citation is warranted, it must issue that citation within 30 days after completing its investigation. However, Figure 7 shows that from 2006 through 2015, Public Health issued more than 1,100 citations at least six months after it identified the deficiencies. This delay is problematic because, according to a Public Health process improvement assessment, a lack of timeliness can have a negative impact on the process of producing a defensible citation.
Additionally, state penalties do not adequately deter facilities from providing substandard care in part because state law reduces a state penalty amount if nursing facilities pay them quickly. Although Public Health assessed more than $28 million in penalties for citations issued from 2006 through 2015, it collected only about $17 million, or 59 percent, of the total amount assessed. The reduced collection amount occurred in part because a nursing facility that does not contest its citation and makes the payment within 15 to 30 days, depending on the type of citation, pays a reduced citation amount. For example, nursing facilities paid penalties for 46 percent of their citations within required time frames and therefore received a 35 percent discount. In addition, nursing facilities appealed an additional 36 percent of all citations, and Public Health subsequently reduced the penalties for 57 percent of the appealed citations. Given the magnitude of these reductions, we are concerned that state law may not create an adequate deterrent for nursing facilities providing substandard quality of care.
Figure 7
From 2006 Through 2015, Public Health Frequently Issued Citations to Nursing Facilities Months After It Identified the Deficiencies

Source: California State Auditor's analysis of Public Health's citation data for inspections ending from 2006 through 2015.
Finally, Public Health did not implement our 2010 audit recommendation that it should adjust penalty amounts for inflation, even though doing so could increase its revenue for quality improvement programs. Specifically, in our June 2010 audit report titled Department of Public Health: It Reported Inaccurate Financial Information and Can Likely Increase Revenues for the State and Federal Health Facilities Citation Penalties Accounts, Report 2010-108, we recommended that Public Health seek legislation authorizing it to revise citation amounts based on the Consumer Price Index. Although in 2011 the Legislature increased the maximum penalty amounts for B citations from $1,000 to $2,000, it last updated penalty amounts for AA and A citations in 2000, and inflation has risen by 46 percent since then. Since October 2013, Public Health has consistently stated in its annual response to our recommendations that the AA and A penalty amounts are adequate and that it will not pursue legislation to increase the penalty amounts. However, if the Legislature revised existing penalty amounts for inflation, a $100,000 fine—the maximum state penalty amount for a violation resulting in patient death—would increase to $146,000. Higher fines that at least increase with inflation are more likely to create a disincentive for providing inadequate patient care.
Legislative Changes Are Necessary to Improve the Quality of Care That Nursing Facilities Provide
As indicated earlier, deficiencies related to substandard quality of care in nursing facilities have increased over the past decade. Nonetheless, evidence suggests that when the State takes action and provides financial incentives, nursing facilities respond by improving the level of care they provide. Therefore, we believe the Legislature should expand upon the State's existing quality incentive program, which provides limited payments to a relatively small number of nursing facilities. Specifically, in addition to continuing the existing program's payments, the State could use a quality assurance fee that nursing facilities currently pay to create new financial incentives that more facilities would receive and that might better motivate these facilities to improve their quality of care.
The State's Quality Program
Entity roles: Public Health scores each nursing facility based on quality-of-care measures, such as nursing hours per patient per day. Public Health provides this information to Health Care Services, which distributes the quality program payments.
Total payment amounts: From fiscal years 2013–14 through 2016–17, the quality program payments to nursing facilities totaled between $88 million and $90 million annually.
Incentive payments: Health Care Services uses 90 percent of the quality program funding to reward nursing facilities that have high overall quality scores. Public Health assigns a score based on a facility's performance against the statewide averages for each quality measure. Health Care Services calculates payments using a tiered system in which only qualified facilities that score more than half the points possible are eligible for payments.
Improvement payments: Health Care Services uses 10 percent of the quality program funding to reward nursing facilities whose incentive scores improved from the preceding year. To qualify for an incentive payment, a nursing facility must rank above the 20th percentile for all qualified facilities.
Current funding: The State funds the quality program through four main sources: General Fund appropriation, penalties Public Health has assessed on facilities for inadequate staffing levels, excess dollars from Medi-Cal's professional liability insurance payments, and federal matching money.
Source: California State Auditor's analysis of the quality program, Public Health's and Health Care Services' quality program webpages, quality program documents, and state law.
Most Facilities Do Not Receive the State's Quality Program Payments
The State's efforts to improve nursing facilities through financial incentives have had a limited effect, in part because the incentives have represented only a small portion of the Medi-Cal funds the nursing facilities receive. Specifically, in 2010 state law required Health Care Services to develop the Quality and Accountability Supplemental Payment System (quality program) to incentivize nursing facilities to implement quality improvements. We summarize the quality program in the text box. However, on average, quality program payments represented only 2 percent of the more than $4 billion in average annual Medi-Cal reimbursements that Health Care Services paid to nursing facilities from fiscal years 2013–14 through 2016–17. For example, for fiscal year 2016–17, Health Care Services issued nursing facilities $88 million in quality program payments, but it paid them more than $4.4 billion in total Medi‑Cal reimbursements.
Moreover, since the State implemented the quality program in 2012, around 66 percent of nursing facilities have been ineligible or did not qualify each year, often because their overall scores were too low or because they received citations from Public Health. As a result, only 191 of about 1,100 nursing facilities qualified for quality program improvement payments in fiscal year 2014–15. More specifically, for fiscal year 2014–15, 23 of the 32 nursing facilities Longwood owned for the entire year were ineligible for program participation or did not qualify to receive program funds. Thus, 72 percent of Longwood's nursing facilities did not receive incentive payments. Similarly, 69 percent of Plum's nursing facilities and 71 percent of Brius's nursing facilities did not receive incentive payments.
Additionally, the quality program does not provide the neediest nursing facilities adequate financial incentives to improve, even though these nursing facilities are more likely to need financial support to invest in quality improvements. According to the quality program coordinator, Public Health is aware that using the incentive scores alone to award quality program payments can result in the distribution of most funds to nursing facilities that are already performing well. To help mitigate this concern, Public Health and Health Care Services also provide improvement payments to nursing facilities whose performance has improved from the previous year. However, Public Health and Health Care Services allocate only 10 percent of total quality program funds toward improvement payments. Therefore, since fiscal year 2013–14, only 17 percent of nursing facilities at most qualified to receive improvement payments, which ranged from a total of $8.8 million to $9 million per year. This amount equated to an average of $49,000 for each of the 180 nursing facilities that received payments in fiscal year 2016–17. Thus, these improvement payments may not be adequate to incentivize nursing facilities with limited resources to make quality-of-care investments, especially if they lack assurance that doing so will result in additional funding. In fact, the quality program coordinator indicated that lower‑performing nursing facilities did not improve enough to qualify for improvement payments for four years.
Ultimately, even though we have concerns about the limited funds the quality program awards and the number of nursing facilities that qualify to participate, evidence indicates that the quality program has resulted in improved quality of care for the metrics it considers. From fiscal years 2013–14 through 2015–16, the quality program considered nine quality-of-care metrics, including the prevalence of pressure ulcers and the percentage of patients who are physically restrained. We found that since the quality program's implementation, the average performance of nursing facilities for each of the nine measures has improved by as much as 50 percent. This performance is a strong indicator that financial incentives can lead to improved quality of care. However, because of the quality program's budgetary limitations, it does not offer a financial incentive for broad-based improvement across all areas of quality of care.
According to the quality program coordinator, the quality program must limit the number of eligible nursing facilities because of budgetary constraints. He further stated that if Public Health increased the percentage of nursing facilities eligible for quality program payments, it would need to reduce the value of those payments, thereby making the incentives less attractive for nursing facility owners.
The Legislature Could Redirect Over $330 Million in Quality Assurance Fees Toward Increased Quality Incentives
The State currently assesses a quality assurance fee on nursing facilities, a significant portion of which it could use for quality improvement incentives. In 2004 the Legislature passed Assembly Bill 1629, which imposed a quality assurance fee on nursing facilities. According to this state law, the quality assurance fee is meant to obtain additional federal funding for the Medi-Cal program, provide additional reimbursements to nursing facilities, and support quality improvement efforts at nursing facilities. Figure 8 shows how the State reimburses nursing facilities for most of their quality assurance fees with no conditions, while it incorporates the remaining funds into the overall funding amount for Medi-Cal. For fiscal year 2016–17, Health Care Services expected to collect $521 million in quality assurance fees from nursing facilities as well as an equal amount of federal matching funds, and it anticipated reimbursing those nursing facilities about $335 million with no conditions. It used the remaining $186 million and the federal matching funds to support the overall Medi-Cal budget; therefore, Health Care Services distributed this funding among all nursing facilities to cover their costs.
Figure 8
The State Returns Most of Nursing Facilities' Quality Assurance Fees to the Facilities Without Condition

Source: California State Auditor's analysis of the Medi-Cal rate-setting methodology and the quality assurance fee.
The State currently uses the quality assurance fee to obtain federal matching funds in order to increase payments to nursing facilities but not to incentivize quality improvements. To this end, when it adopted the regulations to implement the quality assurance fee, Health Care Services accepted a proposal by long-term care stakeholders ensuring that nursing facilities would be refunded a portion of the funds generated by the fee based on the number of Medi-Cal patients in the nursing facilities. If the State instead used the $335 million in quality assurance fees for new quality improvement incentives, the funds could help improve the quality of care throughout the State. If the State had paired this $335 million with the previously discussed $88 million from the quality program payments that the State paid to facilities in fiscal year 2016–17, California would have spent about $423 million for that year on quality incentive programs.
Therefore, the Legislature should amend the law that established the quality assurance fee to require that Health Care Services use quality assurance fees to improve quality of care in nursing facilities rather than return these fees to the facilities without condition. When we shared this finding with Health Care Services, it agreed with the recommendation. The $335 million represents a notable amount of total Medi-Cal nursing facility payments, equaling 8 percent of the total $4.4 billion in rate year 2016–17. In addition, as we show in Table 5, total quality assurance fee payments represent a significant percentage of each company's net income—ranging from 29 percent for Plum to 52 percent for Brius. Consequently, these companies would have a strong incentive to participate in the new program and improve their quality of care in order to continue to receive these funds.
| COMPANY | NET INCOME | QUALITY ASSURANCE FEE PAYMENTS | QUALITY ASSURANCE FEES AS A PERCENTAGE OF NET INCOME | PERCENTAGE OF FACILITIES ABOVE QUALITY THRESHOLD* | QUALITY ASSURANCE FEE PAYMENTS AT RISK† |
|---|---|---|---|---|---|
| Brius | $35.2 | $18.4 | 52% | 25% | $7.4 |
| Longwood | 42.2 | 14.3 | 34 | 28 | 4.9 |
| Plum | 53.8 | 15.5 | 29 | 23 | 3.6 |
Source: California State Auditor's analysis of cost reports, Medi-Cal rate schedules, and Public Health's deficiency data.
Note: Net income numbers come from each company's cost reports for facility fiscal year ending in 2015, quality assurance fee payments are from rate year 2014–15, and the percentages of facilities above the quality threshold comes from 2015 Public Health data.
* We judgmentally selected a threshold of 0.4 F–L deficiencies per bed as the quality threshold for this analysis. Between 2006 and 2015, the number of F–L deficiencies per 100 beds for all California facilities was 0.46. A lower score indicates better performance. In other words, nursing facilities above the quality threshold would not receive quality assurance fee payments under this model.
† For the three companies we reviewed, we calculated the quality assurance fee payments at risk by adding up the total quality assurance fee amounts that Health Care Services expected to return to each nursing facility that exceeded our quality threshold.
Establishing an incentive structure like the one we suggest would likely begin with setting targets for specific quality improvement indicators. For example, the Legislature could set a target of 0.4 F–L deficiencies per 100 beds and subsequently eliminate the reimbursement of the quality assurance fee payment to every nursing facility that did not meet that target. For Brius, this particular target would mean that 20 of its nursing facilities would not have received fee reimbursements totaling $7.4 million in rate year 2014–15 as shown in Table 5, and this amount would have reduced Brius's net income by 21 percent to a total of $27.8 million.
If the Legislature believes that the total elimination of quality assurance fee payments for nursing facilities that do not meet quality improvement targets would be overly burdensome, it could require Health Care Services to reimburse a percentage of the fee—such as 10 percent—without condition and require nursing facilities to meet quality improvement targets as a condition to receive the remaining 90 percent. However, the Legislature also needs to ensure that payment amounts are large enough to incentivize nursing facilities to improve their quality of care.
Although changing how the State distributes quality assurance fees will need CMS's approval, CMS told us that our proposed incentive structure is feasible if the State meets certain requirements. For example, a CMS accountant and fiscal management specialist explained that Health Care Services would need to work with CMS and various stakeholders to develop a new Medi-Cal quality assurance fee reimbursement methodology that meets federal requirements and ensures adequate access to care. However, precedent exists for this policy change; other states, including Indiana, Ohio, and Tennessee, have used funding that was equivalent to quality assurance fees to incentivize quality improvements. Thus, adopting this sort of incentive structure appears to be a viable option for improving quality of care in California.
During our research of other states' quality incentive programs, we identified several best practices for the Legislature to consider. For example, a new quality incentive program in California could follow a model used by Tennessee and have a transition period to allow both the State and nursing facilities to understand how the methodology will affect them. California could also consider offering grants similar to those for a program in Minnesota, in which the state provides funds to supplement the investments that private companies make to improve patient quality of care. Furthermore, a CMS study conducted on states' quality incentive programs recommends that such programs start with goals that most facilities can achieve and then increase its quality standards gradually—an approach that a program in Ohio used. Additionally, the report recommends that states design their new programs so that more facilities can participate and benefit from the incentive payments. Specifically, the new programs should give weight to nursing facilities' improvements toward meeting overall quality standards and reward those facilities that can demonstrate they have made investments toward improving care.
As the State develops these standards, it may identify classes of facilities that should qualify for exceptions. For example, some nursing facilities located in rural regions or owned by small businesses may need to qualify for exceptions because significant reductions in their funding could affect patient access to quality care. The State will also need to ensure that nursing facilities with large numbers of Medi-Cal patients receive enough funding to support their quality improvements because, as we state in the Introduction, Medi-Cal does not cover all the facilities' costs for patient care. Considering that the Legislature must reauthorize the Medi-Cal rate-setting methodology by July 2020, we believe this is an opportune moment to have broad policy discussions with stakeholders regarding how to incentivize quality-of-care improvements in California's nursing facilities.
Recommendations
Legislature
To ensure that Public Health's oversight results in nursing facilities improving their quality of care, the Legislature should do the following:
- Require Public Health to develop by November 2018 a proposal for legislative consideration that outlines the factors it will consider when approving or denying applications from nursing facilities of the same class based on each applicant's ability to provide quality patient care. This proposal should outline the specific criteria—including relevant quality-of-care metrics—that Public Health will consider and the specific thresholds at which higher-level management must approve decisions. Public Health should review its proposal with its stakeholders before forwarding it to the Legislature. The Legislature should codify Public Health's proposal as appropriate.
- Require Public Health to conduct state and federal inspections concurrently by aligning federal and state timelines. Specifically, because federal inspections must occur no later than 15 months since the last federal inspection, the Legislature should require that state inspections occur every 30 months.
- Require that Public Health increase citation penalty amounts annually by—at a minimum—the cost of inflation.
To ensure that the State supports and encourages nursing facilities' efforts to improve their quality of care, the Legislature should modify the quality assurance fee by requiring nursing facilities to demonstrate quality-of-care improvements to receive all or some of their quality assurance fee payments. If nursing facilities do not demonstrate adequate quality-of-care improvements, Health Care Services should redistribute their quality assurance fee payments to those nursing facilities that have improved. In modifying this program, the Legislature should consider the best practices we identified and the feedback that Health Care Services receives from stakeholders.
Public Health
As the Legislature considers changes to state law, Public Health should take the steps necessary to ensure that its oversight results in nursing facilities improving their quality of care by doing the following:
- Amend its application licensing reviews by developing a defined process that specifies how an analyst will determine whether an applicant has demonstrated its ability to comply with state and federal requirements. This process also needs to ensure that analysts conduct complete and standardized reviews of each nursing facility application within each class of facility. Specifically, these processes should clearly outline what factors analysts will consider when determining whether an applicant is in compliance, how analysts will weigh those factors for each class of facility, and what objective thresholds will prompt analysts to elevate applications for review and approval by higher-level management. Additionally, Public Health should document the additional factors higher-level management will consider if applications are elevated for their review to ensure that Public Health conducts standardized reviews of nursing facility applications of the same class. Finally, Public Health should develop processes ensuring that it documents its decisions adequately.
- Ensure that it issues citations in a timely manner, especially for immediate jeopardy deficiencies.
The Net Incomes and Use of Related Parties Rose Over the Past Decade for the Three Companies We Reviewed
Key Points
- The net incomes of the three companies we reviewed increased dramatically over the past decade as they acquired additional facilities.
- Owners of nursing facilities can legally receive income not only through their nursing facilities but also through the related-party businesses they or an immediate family member own or control. We found that the nursing facilities properly disclosed on their annual cost reports 76 of the 80 transactions we reviewed and that Medi-Cal did not pay for any related‑party profits for these transactions.
- Health Care Services has consistently fulfilled its responsibilities related to financial oversight, including conducting on-site audits of nursing facilities and eliminating nonallowable costs from the nursing facilities' cost reports.
Terms Related to Nursing Facility Finances
Net Income—The difference between a nursing facility's revenue and expenses for a given period.
Revenue—The amount a nursing facility earned through its health care operations.
Expense—The amount a nursing facility spent on its health care operations.
Retained Earnings—The accumulated total of the nursing facility's net income minus the amount distributed to its owners.
Distributions—The amount of net income that the nursing facility distributed to its owners during the period.
Source: California State Auditor's analysis of nursing facilities' annual cost reports submitted to Health Planning.
The Net Incomes of the Three Companies We Reviewed Increased Significantly Over the Past Decade
For the three companies we reviewed, our analysis shows that as these three companies grew in size, their net incomes—which the text box defines—increased by tens of millions of dollars. Specifically, as we show in Figure 9, all three companies made less than $10 million in net income in facility fiscal year 2006, but by facility fiscal year 2015 their net incomes had increased to between $35.2 million and $53.8 million. Our analysis showed that the sources of the largest increases in the companies' revenue—and thus the most likely sources of their net incomes—were Medicare and managed care. As we describe in the Introduction, Medi-Cal is not likely to contribute significantly to companies' net incomes because it does not fully cover facilities' costs per Medi-Cal patient. Although the companies' expenses also grew during this period, the increases in their revenue significantly exceeded the growth in their expenses, allowing the companies' net incomes to rise.
Figure 9
Over a 10-Year Period, the Net Incomes of the Three Companies We Reviewed Increased Substantially

Source: California State Auditor's analysis of revenue and expense data from each nursing facility's annual cost reports for the three companies we reviewed.
Note: We define a nursing facility's net income as the difference between the nursing facility's revenue and expenses during a specified period.
Our analysis of the three companies we reviewed indicates that there is a strong statistical correlation between their net incomes and the number of patient beds in their facilities. In other words, these large companies benefit by increasing in scale. Plum increased its number of patient beds by 306 percent from 2006 through 2015, while its net income grew by 682 percent. Similarly, Brius increased its number of patient beds by 1,102 percent during this period, while its net income rose by 604 percent. However, because Brius's increase in patient beds has outpaced its increase in overall net income, the company is unique among the three companies we reviewed in that its net income per bed has decreased from $7,200 per bed in 2006 to $4,200 per bed in 2015. Table 6 shows these changes in the number of patient beds for each company and for the industry statewide from 2006 through 2015. As the three companies we reviewed acquired additional nursing facilities from facility fiscal years 2006 through 2015, the number of patient beds in the rest of the industry decreased.
As net income increased for these three large companies over a 10‑year period, the net income for the rest of the industry in the State decreased dramatically from more than $160 million in net income in facility fiscal year 2006 to less than $75 million in facility fiscal year 2015. It is not entirely clear what caused the decrease in industry net income during this time. We spoke to industry experts, and they noted potential explanations, including changes to Medicare, modifications to nursing facility lease structures, and economic fluctuations. Part of the explanation may also be that as the three large companies we reviewed were expanding, the percentage of California nursing facilities that reported a net loss on their cost reports—those whose expenses outpaced their revenue—increased. Specifically, according to our analysis, 34 percent of nursing facilities not owned by the three large companies we reviewed reported negative net incomes on their cost reports during facility fiscal year 2006. However, by facility fiscal year 2015, this number had increased to 43 percent. In comparison, only 23 percent of Brius's facilities, 3 percent of Longwood's facilities, and 7 percent of Plum's facilities had negative net incomes in facility fiscal year 2015.
| COMPANY | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | TOTAL CHANGE |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Brius | 692 | 1,220 | 1,747 | 2,352 | 3,922 | 4,810 | 5,746 | 6,066 | 6,412 | 8,318 | INCREASE |
| Percentage Increase ↑ or ↓ (Decrease) |
– | ↑ 76% | ↑ 43% | ↑ 35% | ↑ 67% | ↑ 23% | ↑ 19% | ↑ 6% | ↑ 6% | ↑ 30% | ↑ 1,102% |
| Longwood | 3,852 | 3,857 | 3,857 | 3,954 | 3,953 | 3,953 | 3,953 | 3,953 | 3,937 | 4,181 | INCREASE |
| Percentage Increase ↑ or ↓ (Decrease) |
– | 0% | 0% | ↑ 3% | 0% | 0% | 0% | 0% | 0% | ↑ 6% | ↑ 9% |
| Plum | 1,247 | 1,674 | 1,992 | 2,168 | 2,168 | 4,716 | 4,787 | 4,787 | 5,127 | 5,057 | INCREASE |
| Percentage Increase ↑ or ↓ (Decrease) |
– | ↑ 34% | ↑ 19% | ↑ 9% | 0% | ↑ 118% | ↑ 2% | 0% | ↑ 7% | ↓ (1%) | ↑ 306% |
| Other Facilities in the Industry | 102,892 | 101,796 | 100,508 | 99,720 | 98,757 | 95,026 | 94,189 | 93,758 | 92,609 | 91,052 | DECREASE |
Source: California State Auditor's analysis of nursing facility cost report data.
Note: We calculated the number of patient beds using each facility's final cost report each year.
Companies can use their income for a variety of purposes, including retaining their earnings for future investments and paying distributions to owners or investors. Because retained earnings can build over time, they can be significantly higher than a company's annual net income and can go toward such purposes as quality‑of‑care improvements. Plum, for example, had a higher proportion of retained earnings than did Brius or Longwood in facility fiscal year 2015, and Plum also distributed less to its owners, as shown in Figure 10. When we talked to Plum, the chief financial officer stated that this approach was part of the company's investment strategy and that the company has since used a portion of those earnings to invest in 10 additional facilities. In contrast, facilities owned by Longwood distributed $36.1 million of their income to their owners in facility fiscal year 2015, and Brius facilities reported $10.6 million in distributions in that same year.
The Three Companies We Reviewed Earned Income From Related Parties, and This Practice Is Legally Allowable and Common in the Industry
Owners of nursing facilities can legally receive income not only through their nursing facilities, but also through related party businesses they or an immediate family member own or control. Companies that receive Medi-Cal payments may use related-party transactions as long as they disclose the transactions in the annual cost reports that they submit to Health Planning. However, the costs that Medi-Cal reimburses for these transactions can neither include owner profits nor can they exceed the prices of comparable goods or services that could be procured elsewhere. The Introduction explains that related party businesses provide goods or services to a nursing facility. From facility fiscal years 2007 through 2015, the total amount that nursing facilities in California spent on goods and services they purchased from related parties rose 66 percent, from $604.5 million in facility fiscal year 2007 to more than $1 billion in facility fiscal year 2015, according to the annual cost reports the nursing facilities submitted to Health Planning.
The amount that the three companies we reviewed spent on related‑party goods and services also generally rose from facility fiscal years 2007 through 2015, as Figure 11 shows. For example, in facility fiscal year 2015, nursing facilities owned by Plum spent nearly $48 million on goods and services they purchased from related parties, while Brius's nursing facilities spent $65.7 million on purchases from related parties. Brius increased its related-party expenses per patient bed about 600 percent, from $1,100 in facility fiscal year 2007 to $7,900 in facility fiscal year 2015. At the same time, Plum increased its related‑party expenses by more than 155 percent, from $3,700 per bed in facility fiscal year 2007 to $9,500 per bed in facility fiscal year 2015. It is important to note that because nursing facilities and related‑party businesses can have multiple owners, we cannot attribute the entire amounts of any related-party expenses to specific owners based on an analysis of the annual cost reports. Further, we are unable to determine how much of the nursing facilities' related-party expenses represent income for the owners because the cost reports do not include this information, and related-party businesses have their own expenses.
Figure 10
Companies Can Retain Earnings or Distribute Them to Their Owners

Source: California State Auditor's analysis of nursing facilities' annual cost reports.
Figure 11
The Related-Party Expenses for the Three Companies We Reviewed Generally Increased
From Facility Fiscal Years 2007 Through 2015

Source: California State Auditor's analysis of the three companies' related-party expenses from each of their nursing facility's annual cost reports.
Although the revenue earned by these related-party businesses represents additional earning opportunities for their owners, state law ensures that the use of related parties is extremely unlikely to increase the amounts of Medi-Cal payments that nursing facilities receive. An example involving Brius illustrates how owners can make money directly from related parties. In facility fiscal year 2015, Brius's 79 facilities paid a total of $3.5 million to Boardwalk West Financial Services (Boardwalk)—a related party that provides financial consultation services. Further, the two Brius facilities we reviewed in detail paid a total of $108,000 to Boardwalk in facility fiscal year 2015. In the same year, Boardwalk's owner also earned income through owner distributions from Brius's nursing facilities; however, he did not collect a salary from the nursing facilities we reviewed. Our analysis also showed that the owner properly disclosed these related-party transactions and that Medi-Cal has not paid for the costs related to Boardwalk.
Additionally, as Table 7 shows, many of the nursing facilities owned by the three companies we reviewed engaged in related‑party leases. However, under state law, Health Care Services does not pay for leases based on the amounts specified in the leases; instead, as Table 1 in the Introduction shows, it bases the rate it pays for a particular nursing facility's building lease on that facility's age, geographical location, and number of patient beds. This process helps ensure that Medi‑Cal does not pay for potentially inflated lease costs. Table 7 includes lease information reported by nursing facilities owned by the three companies we reviewed.7 In some instances, an operations company—such as the Point Loma nursing facility—leased a property from a related-party property company that owned the building, land, and equipment in question. In other instances, however, a related-party property company leased property from an unrelated party and then subleased the property to a nursing facility operations company, such as the Seaview nursing facility. The use of related-party leases allows companies to receive money from nursing facilities while reducing the facilities' exposure to financial liabilities, such as false claims settlements or punitive damages settlements. Further, according to one of the founders of a company we spoke with, lenders often require that a separate company own the property to protect their lenders' collateral. Regardless of the structure, these related-party leases are allowable, and controls exist to ensure that Medi-Cal does not pay for any potentially inflated lease costs.
Of the three companies we reviewed, Brius alone reported on its annual cost reports interest on related-party loans during the past three years. Specifically, SR Capital and YTR Capital each provided the Brius nursing facilities we reviewed with a revolving line of credit for up to $5 million at 10 percent interest. The total amount of interest the nursing facilities paid varied depending on the outstanding balances; from facility fiscal years 2014 through 2016, the highest amount of total interest we saw for the nursing facilities we reviewed was $10,500. Interest rates for a business's line of credit can vary depending on myriad factors, such as the borrower's credit history, the characteristics of the business, and whether the loan is secured by collateral. Although the nursing facilities might have been able to find lower rates through the open market, the available information suggests that the interest rates for the Brius nursing facilities we reviewed were not unreasonable and were within legal limits. Furthermore, we found that Brius appropriately reported its related‑party loans on its annual cost reports and did not claim the interest for Medi-Cal reimbursement.
When we reviewed a selection of related-party transactions, we determined that the companies we reviewed had properly disclosed in their cost reports the majority of the transactions. Specifically, we selected for the three companies a total of 80 potential related‑party transactions from facility fiscal years 2014 through 2016 to assess whether the companies properly recorded the transactions. We found that the companies properly disclosed 76 of the 80 transactions we reviewed, and we did not find any transactions for which the companies lacked sufficient documentation. Plum disclosed all of its related‑party transactions in its annual cost reports. Brius, on the other hand, did not disclose a related‑party transaction totaling $6,900 in medical equipment rentals. According to a partner at the company that prepares the cost reports for Brius, his company overlooked the transaction, so it was not disclosed as it should have been. However, because Health Care Services eliminated those costs during its annual audit process, the undisclosed transaction has not increased the Medi‑Cal funding that Brius received.
| 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Brius | Number of facilities with related-party leases | NA | NA | NA | NA | 9 | 18 | 32 | 34 | 44 | 67 |
| Percentage of company's facilities with related-party leases | NA | NA | NA | NA | 25% | 40% | 60% | 61% | 75% | 85% | |
| Total spent on related‑party leases* | NA | NA | NA | NA | $6 | $12 | $25 | $29 | $36 | $47 | |
| Plum | Number of facilities with related-party leases | NA | NA | NA | NA | NA | NA | 31 | 33 | 35 | 34 |
| Percentage of company's facilities with related-party leases | NA | NA | NA | NA | NA | NA | 74% | 79% | 80% | 77% | |
| Total spent on related‑party leases* | NA | NA | NA | NA | NA | NA | $6 | $19 | $18 | $18 | |
| Longwood | Number of facilities with related-party leases | 27 | 26 | 27 | 28 | 28 | 29 | 28 | 28 | 28 | 29 |
| Percentage of company's facilities with related-party leases | 84% | 81% | 84% | 85% | 85% | 88% | 85% | 85% | 85% | 81% | |
| Total spent on related‑party leases* | $18 | $18 | $18 | $18 | $20 | $19 | $20 | $19 | $19 | $20 | |
Source: California State Auditor's analysis of Brius, Plum, and Longwood nursing facilities' fiscal years 2006 through 2015 annual cost reports.
NA = The company's facilities did not report any related-party leases in their annual cost reports.
* This total includes lease and rental expenses relating to buildings, equipment, and property improvements.
Additionally, Longwood did not properly disclose a total of three related-party transactions. In two of the three transactions, Longwood did not report accurately the total related-party transaction amounts—$38,200 and $87,900—for facility maintenance and dietician services. According to Longwood's chief financial officer, Longwood facilities only partially reported the expenses to this related party in the related-party reporting fields of the annual cost report, but reported the total expense as an adjustment for Medi‑Cal reimbursement in another page of the cost report. The third improperly disclosed related-party transaction was for $1.5 million in owner salary. Longwood's chief financial officer indicated that he does not know why this payment was not disclosed as a related‑party transaction. However, Longwood eliminated in their submitted annual cost reports these costs for Medi-Cal reimbursements; thus, the failure to disclose the three related‑party transactions did not increase the Medi-Cal funding that Longwood received.
Considerable debate exists about the benefits and drawbacks of related-party transactions. According to nursing home owners, related-party business structures can create efficiencies, reduce the number of disputes with vendors, and minimize taxes, while industry publications have argued that they can reduce liability for the nursing facility owners. However, some advocates for nursing facility residents have contended that related-party transactions obscure the amounts of income that facility owners make and complicate the plight of injured residents who attempt to collect damages through courts. Nevertheless, even though the companies we reviewed have steadily increased their use of related parties in recent years, we found no evidence that these transactions were either illegal or resulted in increased costs to the State. Moreover, we did not identify any significant statistical correlation between the amounts paid to related parties and the quality-of-care indicators we reviewed for the three companies.
Health Care Services Has Fulfilled Its Responsibilities Related to Overseeing Medi-Cal Payments to Nursing Facilities
We analyzed Health Care Services' audits of nursing facilities and related adjustments and found that it performed its audit function adequately. State law requires that Health Care Services audit annually every nursing facility that receives Medi-Cal funds and that it conduct an on-site audit of each facility at least once every three years. During the three-year period we reviewed, Health Care Services had a 99 percent or higher rate of complying with these requirements, and it conducted more than 3,000 audits of more than 1,000 facilities.
Furthermore, during its audit process, Health Care Services eliminated related-party profits and other nonallowable expenses from the Medi-Cal rates it paid the nursing facilities. Table 8 shows our selections of two nursing facilities owned by each of the three companies we reviewed and summarizes how Health Care Services' audits of the facilities' fiscal year 2014 related‑party costs factored into the Medi-Cal rates the State paid the facilities for rate year 2016–17. For example, Plum reported nearly $563,000 in related-party costs in facility fiscal year 2014 for its Redwood Cove facility, but it self-adjusted almost $390,000 of that amount. During its audit process, Health Care Services identified and eliminated another $127,000 of nonallowable related‑party costs, leaving only $46,000 in related-party costs that it included in Redwood Cove's Medi-Cal rate. In another instance, for five Brius facilities we reviewed, Health Care Services eliminated for the three-year period reviewed almost $12 million in claimed costs, $11 million of which was for related-party transactions that Health Care Services determined were not reimbursable.8
| BRIUS | PLUM | LONGWOOD | |||||
|---|---|---|---|---|---|---|---|
| POINT LOMA | SEAVIEW | REDWOOD COVE | VILLA LAS PALMAS | BURBANK HEALTHCARE | MAGNOLIA | ||
Step 1 Nursing facilities reported their total related‑party costs |
↓ | $1,600,900 | $1,028,200 | $562,900 | $859,500 | $1,920,700 | $951,700 |
Step 2 Nursing facilities adjusted their cost reports to remove nonallowable related‑party costs |
− | (1,354,500) | (839,700) | (389,600) | (395,800) | (1,086,300) | (531,200) |
Step 3 Health Care Services audited the cost reports and eliminated additional related‑party costs* |
− | (246,400) | (188,500) | (127,300) | (306,400) | (118,600) | (60,100) |
Sources: California State Auditor's analysis of six nursing facilities' fiscal year 2014 annual cost reports and Health Care Services' audit reports.
* Health Care Services eliminates costs for reasons such as removing related-party profits or because the nursing facility could not provide sufficient documentation.
Although Health Care Services is meeting its obligations related to the audits it conducts, the Legislature could make Health Care Services' process more efficient by requiring nursing facilities that engage related parties in transactions of significant value to submit the related parties' profit and loss statements with the nursing facilities' annual cost reports. Connecticut requires nursing facilities to include in their cost reports a profit and loss statement from each related-party business that received $50,000 or more for goods or services that it provided to the nursing facilities that year. Health Care Services' branch chief of financial audits indicated that requiring nursing facilities to submit such profit and loss statements would assist Health Care Services' auditors—who assess the allowability of costs—in determining the actual costs of related‑party transactions. However, Health Care Services' authority is codified in law, and this change would require legislative action.
Recommendation
Legislature
The Legislature should require nursing facilities to submit annually their related-parties' profit and loss statements to Health Care Services when total transactions exceed a specified monetary threshold. The purpose of these statements would be to assist Health Care Services in its audits.
State Agencies Have Not Always Coordinated Their Oversight Efforts or Ensured the Accuracy and Usefulness of Publicly Available Data
Key Points
- The three state oversight agencies' processes for collecting and auditing or reviewing nursing facility information are duplicative. By increasing their coordination, the agencies could ensure more effectively the best use of resources.
- Health Planning has not ensured that the format of the annual cost reports allows nursing facilities to fully and clearly report information about their related-party transactions. It also has not ensured that nursing facilities report how much they have reinvested into quality-of-care improvements.
- Although Public Health's recently implemented consumer website for researching and comparing nursing facilities is user-friendly, the website does not provide complete and accurate information on nursing facilities' ownership or inspection results, thus impeding consumers' ability to make informed decisions.
The Three State Oversight Agencies' Processes for Collecting, Auditing, and Reviewing Nursing Facility Information Are Duplicative and Inefficient
As Table 9 shows, Health Planning, Public Health, and Health Care Services collect duplicative information related to nursing facility ownership and finances. This replication of effort is inefficient for both the nursing facilities and the State. For example, state law requires nursing facilities to submit their ownership information to Public Health as part of the licensing process, and state regulations also require facilities to submit ownership information to Health Planning. Furthermore, when Public Health receives licensing information from facilities, it manually enters the information into its tracking system and forwards printed copies of nursing facilities' licenses to Health Planning, which then manually enters that license information into its own separate tracking system. Health Planning's program audit manager stated that Health Planning allocates approximately 450 staff hours per year to process the license information for nursing facilities. He also stated that Health Planning would find it beneficial to have electronic copies of license information. According to Public Health, it was not aware that Health Planning wanted electronic copies of license information, but Public Health can provide the electronic licensing information upon request from Health Planning.
Further, two of the State's oversight agencies—Health Planning and Health Care Services—perform audits of duplicative nursing facility information; however, Health Planning's audits fall short of meeting their assigned purpose. State law requires Health Planning to conduct audits on annual cost reports submitted by nursing facilities—it conducts these analyses as desk audits. According to Health Planning's program audit manager, the purpose of the audits is to ensure that the information that the nursing facilities report is uniform, accurate, and complete. However, in our review of Health Planning's audited cost reports, we found that 4,000 of 12,400 audited cost reports, or 32 percent, were incomplete and did not include facility ownership information. According to the program audit manager, some facilities may leave report fields blank when certain reporting requirements do not apply to them. He further stated that when a facility reports certain information improperly in an audited cost report, Health Planning will attempt to address the issue with the report preparer, and, if the issue is not resolved, Health Planning may delete the improperly reported information and instead leave the field blank. Furthermore, Health Planning does not require supporting documentation to verify information reported in the annual cost reports. The program audit manager stated that Health Planning's lack of resources and the number of facilities Health Planning must audit restrict its ability to enforce reporting compliance. As previously discussed, state law also requires that Health Care Services audit annually every nursing facility that receives Medi-Cal funds and that these audits include a review of facility ownership information. Because this ownership review is similar to the information review that is part of Health Planning's desk audits, opportunities exist for these two state agencies to increase coordination.
| Information Collected From Nursing Facilities | HEALTH PLANNING | PUBLIC HEALTH | HEALTH CARE SERVICES |
|---|---|---|---|
| Names of individuals with 5% or more interest | ● | ● | |
| Legal name of the facility | ● | ● | |
| Name of parent company | ● | ● | |
| Names of governing board officers and members | ● | ● | |
| Name of facility administrator | ● | ● | |
| Name of management company | ● | ● | |
| Notification of change of ownership | ● | ● | |
| Number of licensed beds | ● | ● | |
| Revenue and expenses | ● | ● | |
| Documentation supporting related‑party transactions | ● | ● | |
| Tasks Performed by Multiple State Agencies | |||
| Auditing or reviewing ownership information for accuracy | ● | ● | ● |
| Auditing financial information for accuracy | ● | ● |
Source: California State Auditor's analysis of Health Planning's cost reports, Public Health's licensing applications, and Health Care Services' and Health Planning's audit procedures and a selection of their audits.
We believe the three state agencies could increase efficiencies and reduce costs if they reviewed their respective roles and responsibilities to determine whether the current oversight structure is efficient. The review should include an assessment of the potential for increased information sharing and auditing. This type of coordination is not unprecedented. Specifically, Health Care Services has an agreement with Public Health in which Public Health provides Health Care Services information regarding nursing facilities' ownership so that the nursing facilities do not have to provide this information to both state agencies. The three state agencies should develop a working group composed of representatives from each entity to determine how to divide responsibilities most efficiently. When we shared this recommendation with the three state agencies, they did not oppose working together to coordinate these efforts.
Finally, using the information Health Planning and Public Health collect from nursing facilities, the State could create an online dashboard that allows the public to easily understand each nursing facility's and company's quality of care and its financial health. In Figure 12, we present an example of what this dashboard could look like; it shows the financial information and quality-of-care indicators for each of the three companies we reviewed and the rest of the industry. Further, our website (www.auditor.ca.gov) includes an interactive version of this same dashboard. We believe a dashboard of this kind would prove helpful not just to Health Planning, Public Health, and Health Care Services, but also to stakeholders. Furthermore, the transparency and accessibility of the information on the dashboard would enhance the accountability of nursing facilities and their owners and could motivate them to improve their quality of care. Health Planning and Health Care Services agreed that a tool of this kind would be useful; Public Health declined to comment.
Figure 12
The State Could Create an Online Dashboard That Would Allow the Public to Better Understand Nursing Facilities' Financial Health and Quality of Care
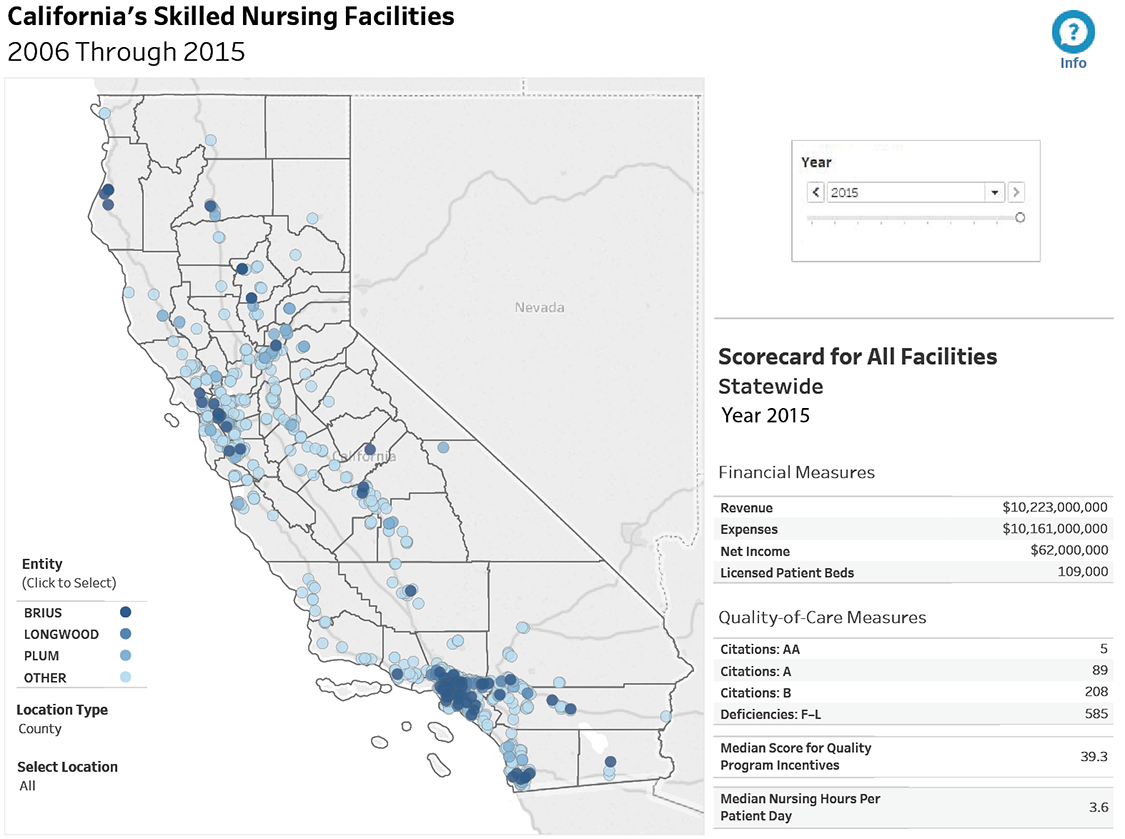
Source: California State Auditor's analysis of nursing facility revenue and expenditure data and of quality-of-care measures.
Note: Our website includes an interactive version of this dashboard. See www.auditor.ca.gov/reports/2017-109/supplemental.html
Health Planning Has Not Ensured That the Format for Annual Cost Reports Allows Nursing Facilities to Clearly Detail Their Related‑Party Transactions
Health Planning can improve the transparency of related-party and nursing facility information by reformatting the annual cost reports that nursing facilities submit. The annual cost report's current format does not always provide stakeholders with sufficient information about the transactions nursing facilities conduct with related parties. Specifically, even though Health Planning requires nursing facilities to report in their annual cost reports all related-party transactions, the cost report template contains only five lines for this information. According to Health Planning, nursing facilities did not often conduct business with related parties at the time it created the cost report template; therefore, five lines were sufficient. However, as the nursing facility industry has evolved and facilities' use of related parties has increased, Health Planning has not amended its form to include additional lines for related-party transactions. Instead, according to Health Planning's program audit manager, it instructs nursing facilities to report the related parties with the largest total transactions and, if necessary, to group together the remaining related-party transactions onto the last line. As a result, understanding all of a nursing facility's related‑party transactions based on its cost reports is often impossible. In fact, we found 1,260, or 10 percent, of 12,430 annual cost reports in which nursing facilities did not completely disclose related-party transactions from 2005 through 2016 because of the limited number of lines. For example, Point Loma reported $177,100 in related‑party transactions in its 2014 cost report by indicating it made payments to a related party for "various" supplies in "various" account titles. However, we found that the nursing facility paid the related party $147,200 for nursing expenses, $26,300 for patient supplies, and $3,600 for food for the facility.
In looking to other states for best practices, we found that Illinois provides related-party supplemental schedules to allow nursing facilities to report all of their transactions involving related entities. To ensure that nursing facilities in California similarly report all related-party transactions, Health Planning should update the cost report template to allow facilities to report an unlimited number of entries. Health Planning agrees with this recommendation and stated that it plans to update the annual cost report format to increase the number of reporting lines for related-party transactions. However, the annual cost-reporting requirements are incorporated in Health Planning's regulations, and changes to the reporting requirements require a regulatory process change.
Furthermore, the current format of the annual cost report makes it difficult for stakeholders—such as the Legislature, families, or other interested parties—to understand how much of a particular related‑party transaction that a nursing facility claimed for Medi‑Cal reimbursement. The current format displays on different report pages the reporting fields for related-party transactions. Specifically, Health Planning requires nursing facilities to report on a separate schedule any adjustments they made to related-party transactions for Medi‑Cal reimbursements, so these adjustments do not appear near the original transactions and do not explicitly state which related-party transactions the facilities adjusted. For example, in its facility fiscal year 2016 cost report, Redwood Cove Healthcare Center (Redwood Cove)—a Plum facility—reported on the related-party schedule a $332,000 related-party transaction for administrative services. It then reported on a different schedule its multiple adjustments to a related-party transaction but did not specify which related-party transaction it had adjusted. According to our analysis, Redwood Cove actually adjusted from $332,000 to $218,000—a decrease of more than $114,000—the amount it claimed for Medi-Cal reimbursement for the specific transaction we reviewed. However, reaching this conclusion took considerable research on our part.
Again, we looked to other states for best practices, and we found that Connecticut requires each nursing facility to report the amount of a related-party transaction next to the amount it has claimed for reimbursement. To provide stakeholders with accessible information about related-party transactions and assurance that Medi-Cal has not paid for related-party profits, Health Planning should update the format of the annual cost report to enable nursing facilities to report on a single schedule the amounts of related-party transactions and the adjustments they made to those amounts. Health Planning agrees with this recommendation, and Health Planning's program audit manager stated that with coordination between Health Planning and Health Care Services, Health Planning can consolidate the information onto a single supplemental page.
Finally, California's current template for annual cost reports does not allow a nursing facility to indicate clearly how much of its net income or retained earnings it reinvests into quality-of-care improvements. For example, although the cost report format provides a field for nursing facilities to report their net incomes, it does not clearly communicate how much of those net incomes facilities have reinvested into quality-of-care improvements. In conjunction with the recommended incentive structure discussed previously, Health Planning should add a schedule to the annual cost report on which nursing facilities must document the amount they reinvest into quality-of-care improvements. This requirement would hold nursing facilities publicly accountable for such reinvestments. However, Health Planning would need to seek a regulatory change to incorporate this schedule in its cost reports. Health Planning's program manager stated that this schedule for nursing facilities could benefit the public and that a similar effort for nonprofit hospitals is in place and can be used as a template for this recommended schedule.
Public Health Does Not Consistently Publish Complete Data, Which Hinders Consumers' Abilities to Reach Informed Conclusions
Although Public Health presently provides information about nursing facilities to consumers through two websites—the historic Health Facilities Consumer Information System (HFCIS) and the new Cal Health Find—the combined information contained on the two websites is not complete. Public Health recently developed Cal Health Find, which will eventually replace HFCIS. Cal Health Find is an innovative and user-friendly resource that incorporates tools that allow consumers to easily search for nursing facilities by location, compare those facilities, view facilities' performance, and file complaints.
However, our review of the completeness of inspection results for nursing facilities available on both HFCIS and Cal Health Find revealed that Public Health does not consistently provide this information on either platform. For example, we were unable to locate on either website two of the 27 inspections, or 7 percent, that we selected for review. In addition, we could not find 13 of the 27 inspections on Cal Health Find. The lack of complete inspection information is problematic because it violates federal requirements that Public Health must provide links to facility inspections on its website, and it also reduces the public's ability to assess the quality of care provided by nursing facilities. The owner of Brius also expressed concerns that in the past Brius has demonstrated to Public Health instances of inaccuracies in the database and therefore he is concerned about the accuracy and reliability of publicly available data.
Moreover, Cal Health Find does not clearly present the chain of ownership in some companies' complex corporate structures, and the information that the website presents can at times be misleading. For example, during our audit, the ownership information that Cal Health Find displayed for the two Plum nursing facilities we reviewed did not indicate that Plum was the parent company for these facilities. Further, Cal Health Find's ownership information for one of Brius's nursing facilities included 35 separate entries, many of which were contradictory or duplicative. For example, the entries indicated that three separate owners collectively held 241 percent ownership interest in one of the facility's parent companies. Ultimately, if Public Health's publicly available data do not allow consumers to discern whether particular companies own nursing facilities, those consumers will lack potentially important information that would allow them to make informed decisions regarding their choices in nursing facilities. When we shared these findings with Public Health, it acknowledged that Cal Health Find has system errors that it still needs to address and stated that HFCIS will continue to be a public resource until these issues are resolved.
Recommendations
Legislature
To improve coordination and efficiency among the state agencies that oversee nursing facilities, the Legislature should require that Health Planning, Public Health, and Health Care Services collaborate to assess the information that each collects from nursing facilities and to develop a proposal by May 2019 for any legislative changes that would be necessary to increase the efficiency of their collection and use of the information. The agencies' goals should include the collection of information by only one agency and the development of a method to share that information with each other. By May 2020, the three agencies should report to the Legislature on the results of implementing their proposal, such as the efficiencies gained through their increased coordination.
To more effectively communicate with consumers about nursing facilities' financial conditions and quality of care, the Legislature should require a state entity—such as Health Planning, Public Health, or Health Care Services—to develop, implement, and maintain for consumers by May 2020 an online dashboard that includes at a minimum information about nursing facilities' net income and quality of care.
Health Planning
To ensure that it provides the public with nursing facility information that is accurate and comprehensible, Health Planning should update its regulations to do the following:
- Append additional schedules to the template for the annual cost report to enable nursing facilities to fully disclose related‑party transactions.
- Provide a single location in the annual cost report template for nursing facilities to enter related-party transaction amounts next to the amounts they are claiming for Medi-Cal reimbursement.
- Create an additional schedule in the cost report template that depicts how a company is investing in quality‑of‑care improvements.
Public Health
To improve the availability and transparency of information, Public Health should upload all inspection findings to Cal Health Find and review ownership data by May 2019.
OTHER AREAS WE REVIEWED
To further address the audit objectives included in Table 13, we examined the subject areas discussed below. We present here the results of our review as well as any associated recommendations that we have not previously discussed.
Peer Groups That Health Care Services Uses to Cap Certain Medi‑Cal Rates
Health Care Services continues to use peer groups, which were established more than a decade ago using limited data, to cap certain Medi-Cal rates paid to nursing facilities. However, we found that the rate caps can be increased by companies that have both higher costs and a large market share of the nursing facilities in particular peer groups, and these increases can affect payments for all nursing facilities in that peer group. State law requires that Health Care Services calculate the portions of the Medi-Cal rates for nursing facilities related to five of the seven cost categories by grouping the facilities into county-specific peer groups, as we describe in Table 1 in the Introduction. To meet this requirement, Health Care Services created seven peer groups in 2005 based on a consultant's report that used limited cost data from 2003 for nursing facilities. Specifically, the consultant's report looked only at direct care costs, and it did not look at other costs, such as administrative and indirect care costs. Currently, the peer groups range in size from fewer than 20 to more than 300 nursing facilities. These peer groups are used to implement cost controls that we refer to as rate caps. The actual amounts of the rate caps depend on the costs of the facilities within each peer group. Higher rate caps in a peer group can lead to increased Medi-Cal payments for high-cost facilities. However, low-cost facilities will continue to receive rates based on their actual costs because those costs will fall below the rate cap.
In reviewing these peer groups, we observed that a large company with significant market share could affect Medi‑Cal rates for multiple peer groups. For example, we observed that because Plum purchased 28 nursing facilities in 2011, all of its facilities had above‑average administrative costs in the years that followed. Because Plum had a significant market share in four peer groups, its higher administrative costs increased the Medi‑Cal rate caps for those four peer groups, and as a result Plum received higher Medi-Cal payments. For example, in one peer group, Plum received in excess of $10 million in additional Medi-Cal payments over a four‑year period as a result of its higher administrative costs increasing the rate cap for that peer group. However, other companies that do not have large market shares within their peer groups are not paid for similar increases in their administrative costs because their costs do not influence the caps to the same degree. To address this inequity, Health Care Services should update its peer groups with more recent and more complete information, and it should revise its peer group methodology to consider the potential impact of industry consolidation—which is occurring for the three companies we reviewed. Health Care Services agreed that it should update its peer groups.
Recommendation
Health Care Services should use current data to revise and update the peer groups it uses to set Medi-Cal rates. In doing so, it should take into consideration the consolidation of the nursing facility industry.
Additional Data Requested by the Audit Objectives
The nursing facilities owned by the three companies we selected—Brius, Plum, and Longwood—all used related-party financial or administrative services in facility fiscal years 2014 through 2016, as Table 10 shows.
Table 10
Nursing Facilities Owned by Brius, Plum, and Longwood Used Related Parties for Administrative and Financial Services
| COMPANY | RELATED PARTY FOR ADMINISTRATIVE AND FINANCIAL SERVICES | NUMBER OF EMPLOYEES | 2014 | 2015 | 2016 |
|---|---|---|---|---|---|
| Brius† | Boardwalk | 4 | ● | ● | ● |
| SR Capital | 0‡ | ● | ● | ● | |
| YTR Capital | 0‡ | ● | ● | ||
| Plum | Plum Healthcare Group | 187 | ● | ● | ● |
| Longwood | Longwood Management Corporation | 133 | ● | ● | ● |
Source: California State Auditor's analysis of annual cost reports and company employee records for facility fiscal years 2014 through 2016.
* Numbers represent company employee counts as of facility fiscal year 2016.
† Many Brius facilities use a large administrative services company that is comparable to Plum Healthcare Group and Longwood Management Corporation. Health Care Services and Brius are currently in litigation regarding whether this administrative services company is a related party.
‡ SR Capital and YTR Capital are owner-managed companies that use contract employees.
Table 11 compares the leases for Brius's, Plum's, and Longwood's facilities to the leases for facilities owned by other companies in the same counties in facility fiscal year 2015. According to the chief financial officer of Rockport Healthcare Services (Rockport), a limited liability company that provides administrative services to the Point Loma nursing facility, Point Loma's annual lease per patient bed is more expensive than are other facilities' leases in the same county because of Point Loma's location and recent facility renovations. Additionally, Brius owned and operated all of the nursing facilities in Humboldt County in facility fiscal year 2015. However, as discussed earlier, Medi-Cal does not reimburse the cost of a nursing facility lease based on the amount specified on the lease; instead, Medi-Cal uses a formula that takes into account the age of the facility, its geographical location, and its number of patient beds.
| COMPANY | FACILITY | COUNTY | ANNUAL LEASE AMOUNT PER BED FOR THE IDENTIFIED FACILITY | COMPANY'S ANNUAL LEASE AMOUNT PER BED IN THIS COUNTY FOR ALL OF ITS FACILITIES | ANNUAL LEASE AMOUNT PER BED FOR OTHER FACILITIES IN THE COUNTY |
|---|---|---|---|---|---|
| Brius | Point Loma* | San Diego | $10,800 | $8,900 | $6,800 |
| Seaview* | Humboldt | 8,700 | 8,700 | 8,700† | |
| Plum | Redwood Cove* | Mendocino | 3,900 | 3,900 | 3,800 |
| Villa Las Palmas | San Diego | 4,000 | 4,900 | 6,800 | |
| Longwood | Burbank Healthcare* | Los Angeles | 6,000 | 5,600 | 5,600 |
| Magnolia* | Los Angeles | 5,400 | 5,600 | 5,600 | |
Source: California State Auditor's analysis of nursing facilities' audited annual cost reports for facility fiscal year 2015.
* The facility leased property from a related party.
† All other facilities in the county are Brius-owned facilities.
Finally, from facility fiscal years 2014 through 2016, selected nursing facilities owned by Brius, Plum, and Longwood engaged in related‑party transactions that represented 14 percent to 25 percent of their nonpayroll expenses, as Table 12 shows.
| BRIUS | PLUM | LONGWOOD | ||||
|---|---|---|---|---|---|---|
| FACILITY FISCAL YEAR | POINT LOMA | SEAVIEW | REDWOOD COVE | VILLA LAS PALMAS | BURBANK HEALTHCARE | MAGNOLIA |
| 2014 | 20% | 25% | 23% | 15% | 21% | 23% |
| 2015 | 21 | 24 | 21 | 14 | 17 | 22 |
Source: California State Auditor's analysis of nursing facilities' fiscal years 2014 and 2015 audited annual cost reports.
SCOPE AND METHODOLOGY
The Joint Legislative Audit Committee (Audit Committee) directed the California State Auditor to conduct an audit of California's oversight of nursing facilities. During this audit, we were to examine the method by which the State sets Medi-Cal rates for nursing facilities and the degree to which the facilities' quality of care affects Medi-Cal payments. The Audit Committee also asked us to evaluate the use of related-party entities and transactions by nursing facilities, including those facilities owned by or related to Brius. The analysis that the Audit Committee approved contains 10 objectives. We list these objectives and the methods we used to address them in Table 13.
| AUDIT OBJECTIVE | METHOD | |
|---|---|---|
| 1 | Review and evaluate the laws, rules, and regulations significant to the audit objectives. | Reviewed relevant laws, regulations, and other significant background materials applicable to state and federal oversight of skilled nursing facilities* and to related‑party business transactions. |
| 2 | Assess the roles and responsibilities of relevant state agencies—including Health Planning, Health Care Services, and Public Health—that oversee nursing facility financial reporting, collect a variety of health facility data, set Medi‑Cal rates and reimbursements, audit compliance with reporting requirements, and ensure and enforce quality of care. Determine whether there is effective coordination among these entities. |
|
| 3 | Evaluate whether the policies, processes, and practices for establishing rates and/or reimbursements for nursing facilities are reasonable and appropriate. Specifically, for the most recent three years, to the extent possible, assess whether related‑party transactions affect Medi‑Cal rate and reimbursement policies, practices, and processes. |
|
| 4 | For a selection of the related‑party transactions covering the past three years for both Brius’s nursing facilities and for a comparable company’s nursing facilities, do the following to the extent possible: a. Assess the total dollar amount of related‑party transactions, the amount of related‑party transactions reimbursed by Medi‑Cal, and the percentage of nonpayroll expenses these transactions represent. b. Determine the number of related‑party businesses that performed any sort of financial transactions with the nursing facilities and what services, goods, or supplies these related parties provided. Determine which related parties had the most transactions in terms of dollar value. c. Evaluate the number of nursing facilities engaged in related‑party transactions for the purpose of leasing buildings, property, and/or equipment. Determine the dollar amount for these transactions and compare those amounts to the amounts paid in transactions with unrelated parties and to market rates for similar purposes. d. On a county‑by‑county basis, determine the difference in the annual lease per nursing home bed paid by selected facilities versus unselected nursing facilities. |
|
| 5 | To the extent possible, for the most recent three years using the selection identified in Objective 4, do the following: a. Determine whether related‑party transactions comply with relevant laws and regulations in addition to being reasonable. Assess whether related‑party transactions were properly reported and whether available records indicate the ownership of related parties. b. Assess whether the terms and conditions of related‑party transactions are memorialized in written contracts. c. Determine how many nursing facility owners engaged in related‑party transactions to lease buildings. d. Identify and assess the financial services that related parties provide to the nursing facilities and the number of employees these related parties employ. Assess how common it is for nursing facilities and other related businesses to purchase financial services from related parties. e. With respect to related parties that have extended loans and credit to the selected nursing facilities, evaluate whether the interest rates charged by the related parties are fair and reasonable and comply with relevant laws, regulations, and contract provisions. |
|
| 6 | Determine how quality of care can impact Medi‑Cal payments to nursing facilities. For the selection of nursing facilities identified in Objective 4, assess the effectiveness of state agency oversight and monitoring of these facilities. |
|
| 7 | Evaluate the effectiveness and comprehensiveness of Health Planning’s annual reporting form and the department’s associated policies and protocols to determine whether these disclosure tools are adequate for monitoring nursing facility related‑party transactions and for safeguarding taxpayers from abuse and fraud. To the extent possible, do the following: a. Assess whether the financial reporting requirements allow for collection of adequate information on related‑party transactions. b. Determine whether the form provides sufficient information regarding whether related‑party transactions create a conflict of interest or exceed area market prices. c. Evaluate whether sufficient transparency and accountability safeguards exist to identify and prevent conflicts of interest, fraud, and abuse. |
|
| 8 | Assess what audits and investigations state agencies perform related to nursing facility related‑party transactions. Ensure audits and investigations are being performed as required and are adequate for their purposes. |
|
| 9 | Identify any best practices from other states regarding approaches to enhancing the transparency of nursing facility related‑party transactions including an assessment of related‑party transaction legislation passed in 2013 in Connecticut. | Researched other states, such as Connecticut and Illinois, to determine best practices in establishing nursing facility transparency. |
| 10 | Review and assess any other issues that are significant to the audit. | Obtained and analyzed financial data from Health Planning’s nursing facility annual cost reports for facility fiscal years 2006 through 2015 to determine nursing facility revenues, expenses, net income, retained earnings, and distributions. In some cases, we presented financial information in the report beginning in facility fiscal year 2007 because that was the first full year that Brius operated nursing facilities in California. |
Sources: California State Auditor’s analysis of audit request number 2017‑109 and information and documentation identified in the table column titled Method.
* We have limited our review to free‑standing nursing facilities that are not part of a hospital.
Assessment of Data Reliability
In performing this audit, we obtained electronic data files extracted from the information systems listed in Table 14. The U.S. Government Accountability Office, whose standards we are statutorily required to follow, requires us to assess the sufficiency and appropriateness of computer‑processed information that we use to support findings, conclusions, or recommendations. Table 14 describes the analyses we conducted using data from these information systems, our methods for testing, and the results of our assessments. Although these determinations may affect the precision of the numbers we present, there is sufficient evidence in total to support our audit findings, conclusions, and recommendations.
| DATA SOURCE | PURPOSE | METHOD AND RESULT | CONCLUSION |
|---|---|---|---|
| Health Care Services Medi‑Cal rate schedules |
To document Medi‑Cal rates, audited costs, and market share for selected companies and facilities for four rate years. | We performed completeness and accuracy testing. We compared the number of nursing facilities to the number of nursing facility‑specific rates and verified the rate calculations for each year we reviewed and did not identify any issues. | Sufficiently reliable for the purposes of this audit. |
| Health Care Services Financial Audits Tracking System |
To document the audits that Health Care Services performed on nursing facilities for three years. | We performed completeness and accuracy testing. We compared the number of nursing facility audits that Health Care Services should have performed against what it documented it performed and did not identify any significant issues. We also performed accuracy testing for 15 audits related to the three companies we reviewed and did not identify any significant issues. Through our review we discussed the minor issues that we identified with Health Care Services and determined there was no impact on our audit conclusions. | Sufficiently reliable for the purposes of this audit. |
| Health Planning Cost report data for the period December 31, 2005, through December 30, 2016 |
To evaluate various financial and staffing measures for nursing facilities and analyze related‑party transactions. | We performed data‑set verification procedures and electronic testing of key data elements and did not identify any issues. We did not perform accuracy and completeness testing on these data because the information is self‑reported and source documents are stored at various locations throughout the State, making such testing cost‑prohibitive. |
Although we did not perform a full data reliability assessment, there is sufficient evidence in total to support our findings, conclusions, and recommendations. |
| Longwood Longwood Management Corporation’s general ledgers for facility fiscal years 2014 through 2016 |
To perform related‑party transaction testing for selected transactions from Longwood facilities. | We performed completeness and accuracy testing. We compared the general ledgers to the income statements for selected nursing facilities and did not identify any material discrepancies. We also obtained supporting documentation for the related‑party transactions we reviewed and did not identify any material differences between the supporting documentation and the general ledger entries. | Sufficiently reliable for the purposes of this audit. |
| Plum Plum’s general ledgers for facility fiscal years 2014 through 2016 |
To perform related‑party transaction testing for selected transactions for Plum nursing facilities. | We performed completeness and accuracy testing. We compared the general ledgers to the income statements and balance sheets for selected facilities and did not identify any material discrepancies. We also obtained supporting documentation for the related‑party transactions we reviewed and did not identify any material differences between the supporting documentation and the general ledger entries. | Sufficiently reliable for the purposes of this audit. |
| Public Health ASPEN data from January 1, 2006, through December 31, 2016 |
To identify nursing facility federal deficiencies and state relicensing inspections. | We performed data‑set verification procedures and electronic testing of key data elements and did not identify any issues. We performed accuracy testing. Specifically, we reviewed key data elements for 30 inspections that we selected based on the type of the inspection and inspection dates. For those inspections we verified certain dates, the scope and severity of selected deficiencies, and the regulatory violations associated with those deficiencies to ensure the data matched survey documents. We did not identify any significant issues. We did not perform completeness testing because source documents are stored at various locations throughout the state, making such testing cost‑prohibitive. |
Although we did not perform a full data reliability assessment, there is sufficient evidence in total to support our findings, conclusions, and recommendations. |
| Public Health Quality and Accountability Supplemental Payment program reports from fiscal years 2012–13 through 2015–16 |
To evaluate various quality‑of‑care measures for facilities for fiscal years 2012–13 through 2015–16. | We performed data‑set verification procedures and electronic testing of key data elements and did not identify any issues. |
Although we did not perform a full data reliability assessment, there is sufficient evidence in total to support our findings, conclusions, and recommendations. |
| Public Health ELMS data from January 1, 2006, through December 31, 2015 |
To identify nursing facility citations from 2006 through 2015. | We performed data‑set verification procedures and electronic testing of key data elements and did not identify any issues. We did not perform accuracy and completeness testing on these data because source documents are stored at various locations throughout the State, making such testing cost‑prohibitive. |
Although we did not perform a full data reliability assessment, there is sufficient evidence in total to support our findings, conclusions, and recommendations. |
| Rockport Rockport’s general ledgers for facility fiscal years 2014 through 2016 |
To perform related‑party transaction testing for selected transactions for Brius facilities. | We performed data‑set verification and electronic testing of key data elements and did not identify any issues. We also performed completeness and accuracy testing. We compared the general ledgers to the income statements and balance sheets for selected facilities and we did not identify any material discrepancies. We also obtained supporting documentation for the related‑party transactions we reviewed and did not identify any material differences between the supporting documentation and the general ledger entries. | Sufficiently reliable for the purposes of this audit. |
| Secretary of State’s Office Automated Corporation System and Limited Partnership/Limited Liability Company System |
To identify people and addresses associated with businesses. | We performed data‑set verification procedures and electronic testing of key data elements and we did not identify any issues. To test the accuracy of the data, we traced key data elements for a selection of companies to supporting documentation and found the data to be accurate. To test the completeness of the data, we traced a haphazard selection of companies from the website of the Secretary of State’s Office to the data and found the data to be complete. |
Sufficiently reliable for the purposes of this audit. |
Source: California State Auditor’s analysis of various documents, interviews, and data from the entities listed in the table.
We conducted this audit under the authority vested in the California State Auditor by Section 8543 et seq. of the California Government Code and according to generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives specified in the Scope and Methodology section of the report. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Respectfully submitted,
ELAINE M. HOWLE, CPA
State Auditor
Date:
May 1, 2018
Staff:
Kathleen Klein Fullerton, MPA, Audit Principal
Kathryn Cardenas, MPPA
Inna A. Prigodin, CFE
David F. DeNuzzo, MBA
Jamie A. Pritchard, MIA
Matt Gannon
Michael Tejada
IT Audits:
Kim L. Buchanan, MBA, CISA
Grant Volk, MA, CFE
Sarah Rachael Black, MBA, CISA
Legal Counsel:
Heather Kendrick, Sr. Staff Counsel
For questions regarding the contents of this report, please contact
Margarita Fernández, Chief of Public Affairs, at 916.445.0255.
Footnotes
4 We did not perform on‑site procedures to test the quality of care in nursing facilities. Rather, we reviewed Public Health’s oversight of quality of care in part through analyzing federal deficiencies and state citations that Public Health issued as part of its enforcement responsibilities. Deficiencies and citations are two of several quality‑of‑care indicators that can be measured, but we focused our review on these indicators due to their direct connection to Public Health’s ongoing oversight responsibilities. We discuss other quality‑of‑care indicators we reviewed throughout this section. Go back to text
5 We focused our review on AA, A, and B citations because they are the most egregious. Therefore, when we use the term citation in this report, we are referring to these specific citation types. Go back to text
6 The term class of facility refers to facilities that are similarly situated. In other words, Public Health could use a standardized approach for facilities in a particular class because those nursing facilities share significant characteristics, such as their financial health or the sizes of their facilities in terms of patient beds. Go back to text
7 Leases may include assets, such as buildings, equipment, property improvements, and land. Go back to text
8 Brius and Health Care Services are disputing adjustment amounts. Go back to text