Audit Results
The State Provides Fragmented Oversight and Inconsistent Guidance Related to the Disposal of Home‑Generated Sharps and Pharmaceutical Waste
The State does not assign oversight responsibility to a specific agency for the disposal of home‑generated sharps and pharmaceutical waste, resulting in consumers’ receiving a patchwork of inconsistent messages regarding proper disposal methods. In fact, when we reviewed relevant consumer guidance from federal, state, and local agencies, we identified a number of messages that directly contradict one another. These inconsistent messages increase the risk that consumers will dispose of home‑generated sharps and pharmaceutical waste in illegal, unsafe, or environmentally harmful ways. Further, these mixed messages emphasize the need for a single oversight agency in California to unify the differing guidance on how to dispose of home‑generated sharps and pharmaceutical waste.
Several government agencies have oversight of sharps disposal, depending on the disposal method. Since September 2008, state law has specifically prohibited California residents from disposing of sharps waste in the trash. As the text box discusses, the medical waste act outlines four types of facilities that may collect home‑generated sharps waste: household hazardous waste facilities, home‑generated sharps consolidation points, medical waste generator facilities, or facilities that receive the sharps through mail‑back containers. The authority to approve each of these facilities varies, and different entities can have authority over the same facilities. For example, three entities oversee household hazardous waste sites: counties and city governments establish the sites; under state law, Toxic Substances Control issues permits to the sites; and CalRecycle requires that the sites report their collection data to it. These different levels of authority create complexity in the disposal process.
Adding to this administrative complexity, state law classifies sharps waste differently depending on where consumers dispose of it. For example, the medical waste act specifically excludes home‑generated sharps waste from its definition of medical waste. However, it grants Public Health the authority to approve consolidation points, which are locations—such as police stations and pharmacies—that collect home‑generated sharps waste. Further, the medical waste act states that waste these consolidation points collect must be treated as medical waste, which means that, unless certain exceptions apply, the entities that haul it must be registered with Toxic Substances Control and listed with Public Health, which must approve any entities that haul and treat this waste. After processing, the sharps waste becomes solid waste and, as a result, oversight for it transfers to CalRecycle.
In contrast to the State’s complex rules regulating the disposal of sharps, a defined regulatory framework for home‑generated pharmaceutical waste in California does not exist. Because home‑generated pharmaceutical waste is generally exempt from federal hazardous waste and state medical waste regulations, residents may legally dispose of it in the trash in most cases. However, federal regulation does restrict the collection of pharmaceutical waste that contains controlled substances to law enforcement and DEA registrants, such as hospitals and pharmacies. Further, since distinguishing controlled substances from other types of drugs in pharmaceutical waste can be difficult, collection receptacles often must follow the federal restrictions as a standard practice for all pharmaceutical waste.
In part because of the lack of clear regulations and oversight, the State does not provide a unified statewide message for the disposal of home‑generated sharps or pharmaceutical waste, increasing the likelihood of improper disposal. When we reviewed federal and state agencies’ websites to determine the nature of the guidance they provide, we found that the guidance varies significantly. In fact, certain agencies provide guidance that directly contradicts the guidance offered by other agencies. Further, in some instances, federal guidance conflicts with state guidance.
As Figure 4 shows, state and federal agencies provide a number of different messages regarding the disposal of pharmaceutical waste. For instance, most state agencies recommend that consumers use official collection programs for pharmaceutical disposal. Alternatively, some federal and state agencies recommend disposing of pharmaceuticals in the trash after mixing them with an undesirable substance and sealing them in a plastic bag. Because neither state law nor federal regulation differentiates home‑generated pharmaceutical waste from solid waste, consumers’ disposing of their personal pharmaceuticals in their trash is legal. However, a risk exists that the pharmaceuticals in landfills will leach into groundwater. Additionally, when a disposal site is not available, the U.S. Food and Drug Administration (FDA) recommends that consumers flush unused medications that contain controlled substances to avoid the possibility that individuals other than the patients will take the medications. This guidance directly contradicts guidance from Public Health and the federal Centers for Disease Control and Prevention, which states that consumers should not flush medications. CalRecycle says consumers should not flush unused medications except for those on the FDA’s list because waste treatment plants are not designed to remove pharmaceutical compounds.
Figure 4
State and Federal Agencies Suggest Ways to Dispose of Home‑Generated Sharps and Pharmaceutical Waste

Source: California State Auditor’s analysis of federal and state agencies’ messages about proper disposal of home‑generated sharps and pharmaceutical waste.
Federal and state agencies send mixed messages about the disposal of home‑generated sharps waste as well. CalRecycle and Public Health both recommend that consumers dispose of sharps waste in approved sharps containers at approved collection sites to reduce risks of disease transmission and needle sticks. However, when consumers do not have access to approved sharps containers, the FDA recommends putting sharps in heavy plastic containers, such as empty laundry soap containers, but transporting sharps in those containers is illegal in California, if the local enforcement agency has not approved the container. Conflicting and inconsistent messages among federal and state agencies may create confusion for consumers and thus increase the risk that they will not dispose of their sharps in a safe and environmentally responsible manner.
If the State placed with a single oversight agency the responsibility for guiding consumers’ disposal of sharps and pharmaceutical waste, that agency could work with federal and state agencies to create a unified educational campaign promoting consistent and proper disposal methods. Nonprofit organizations, local government agencies, and other states have developed public information campaigns regarding the proper disposal of home‑generated sharps and pharmaceutical waste, but California has not yet employed such a strategy. We discuss sharps and pharmaceutical disposal programs from other states and countries later in this report.
Because CalRecycle already oversees all of California’s state‑managed, solid waste‑handling programs as well as its specialized recycling programs, it may be best‑positioned to oversee household pharmaceutical and sharps waste disposal. Although other agencies currently oversee home‑generated sharps and pharmaceutical waste in certain situations, CalRecycle has a role in nearly every disposal method because it has oversight of landfills, incinerators, and processing stations. The chief of CalRecycle’s Statewide Analytical Resources Branch of its Materials Management and Local Assistance Division (analysis branch chief) does not believe CalRecycle is the best agency to oversee sharps and pharmaceutical waste disposal because it has no expertise in proper medical waste disposal or the enforcement of laws requiring proper disposal. However, the amount of medical expertise required to operate a collection program for sharps and pharmaceuticals seems minimal because the program would focus on disposal rather than consumption. In addition, CalRecycle already has oversight of sharps when they are sent to landfills after being sterilized, and it has oversight of the three incinerators in the State that can destroy pharmaceutical waste.
In addition, we noted a number of reasons why other state agencies are not as well‑suited as CalRecycle to provide oversight and management of collection and disposal programs for home‑generated sharps and pharmaceuticals. For example, CalRecycle’s analysis branch chief suggested either Public Health or the Pharmacy Board as alternatives because these two agencies do possess medical expertise. However, Public Health is not well‑suited for this role because it lacks CalRecycle’s experience in managing waste collection and disposal programs. Further, the Pharmacy Board is not a suitable option because it exists to ensure quality pharmacist care and the appropriate use of pharmaceuticals. Additionally, the Pharmacy Board regulates and licenses pharmacies. Toxic Substances Control is also an inappropriate choice because it performs only permitting functions for just one type of collection site—household hazardous waste facilities. In addition, Toxic Substances Control’s mission is to restore contaminated resources and reduce hazardous waste generation—not to collect or dispose of home‑generated sharps and pharmaceutical waste.
Although Most Consumers Have Reasonable Access to Free Collection Sites for Sharps and Pharmaceutical Waste, They May Not Be Aware of the Sites’ Locations
Eighty‑nine percent of Californians—almost 34 million people—live within a 20‑minute drive of free collection sites for both home‑generated sharps and pharmaceutical waste. According to our analysis of California’s census data and collection site addresses, access to free collection sites is broadest in the State’s metropolitan areas. However, because the State does not communicate accessible, reliable information, many consumers may not be aware of available collection sites. A primary problem is that no state agency maintains accurate and complete information on collection sites. To address this problem, the Legislature should task CalRecycle with creating, maintaining, and publicizing an accurate list of collection sites in California.
The remaining four million Californians may lack reasonable access to either sharps waste collection sites, pharmaceutical waste collection sites, or to both. In particular, access to disposal sites is often limited in more rural or isolated parts of the State. To ensure that consumers in these areas have the ability to properly dispose of sharps and pharmaceutical waste, the State could subsidize these consumers’ use of prepaid mail‑back envelopes, among other options.
Most Consumers in Urban Areas Have Access to Disposal Sites for Home‑Generated Sharps and Pharmaceutical Waste
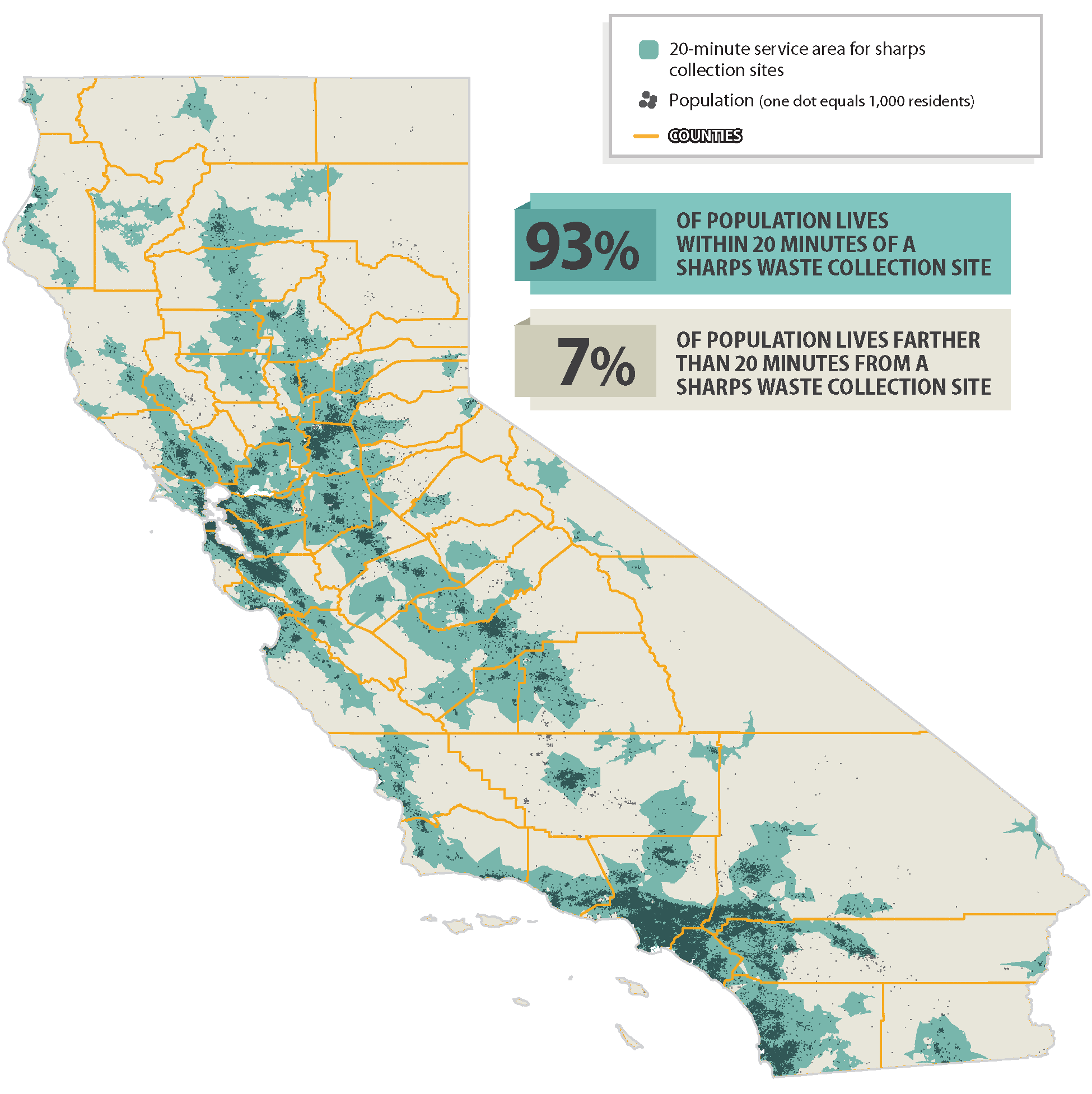
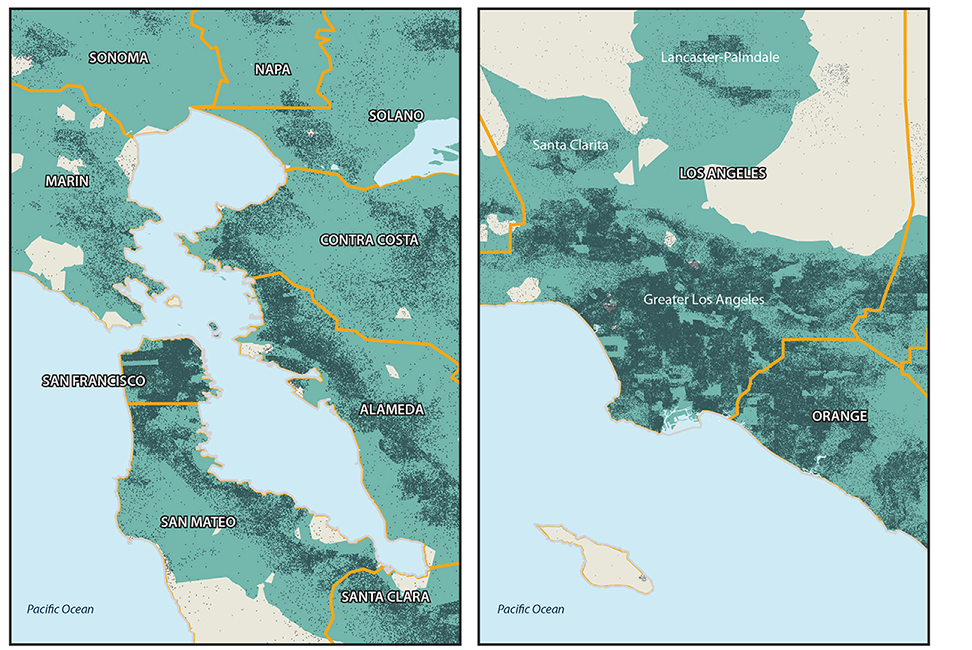
As Figure 5 shows, nearly 35.4 million Californians, or 93 percent of all residents, live within a 20‑minute drive of free sharps collection sites. We refer to this proximity to collection sites as reasonable access, though we recognize that consumers use varying types of transportation.1 In particular, consumers who live in urban areas of the State generally have reasonable access to sharps collection sites. For example, as Figure 6 demonstrates, nearly the entire population of Los Angeles County lives within a 20‑minute drive of sharps collection sites. Figure 6 also shows that the San Francisco Bay Area also has broadly accessible sharps collection sites: in fact, 99.6 percent of the population in San Francisco lives within a 20‑minute drive of sites. This high level of reasonable access is likely the result of the San Francisco Safe Needle Disposal Program, which San Francisco established in 1991 to provide free disposal of home‑generated sharps at every Walgreen Co. (Walgreens) pharmacy—and at certain other locations—in the city.
Click here for a closer look at Figure 5.
Figure 5
State and Federal Agencies Suggest Ways to Dispose of Home‑Generated Sharps and Pharmaceutical Waste
Source: California State Auditor’s analysis of federal and state agencies’ messages about proper disposal of home‑generated sharps and pharmaceutical waste.
Figure 6
State and Federal Agencies Suggest Ways to Dispose of Home‑Generated Sharps and Pharmaceutical Waste

Source: California State Auditor’s analysis of federal and state agencies’ messages about proper disposal of home‑generated sharps and pharmaceutical waste.
In contrast, less populated areas of the State lack reasonable access to sharps collection sites. Rural areas with a low population density are likely to have few, if any, collection sites, and small urban areas, are also more likely to have limited access. For instance, our analysis found that around one‑third of Kern County (Kern) residents—282,000 people—live outside a 20‑minute drive from sharps collection sites. Figure 6 demonstrates that while Kern’s largest city, Bakersfield, contains permanent collection sites, smaller urban areas like Delano, Wasco, and Taft do not. Therefore, to dispose of sharps waste, residents in these areas may have to drive long distances or rely on periodic collection events.
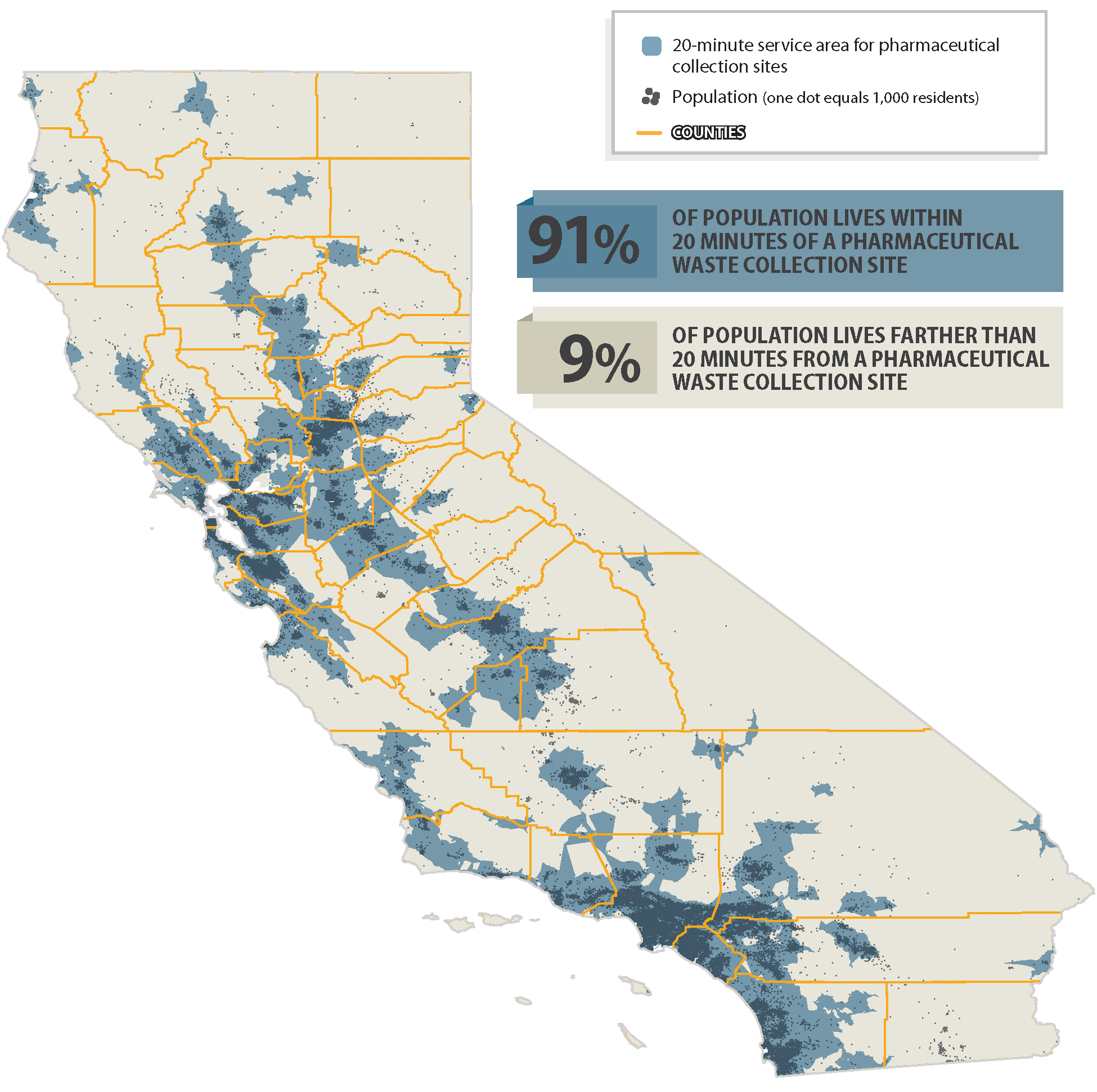
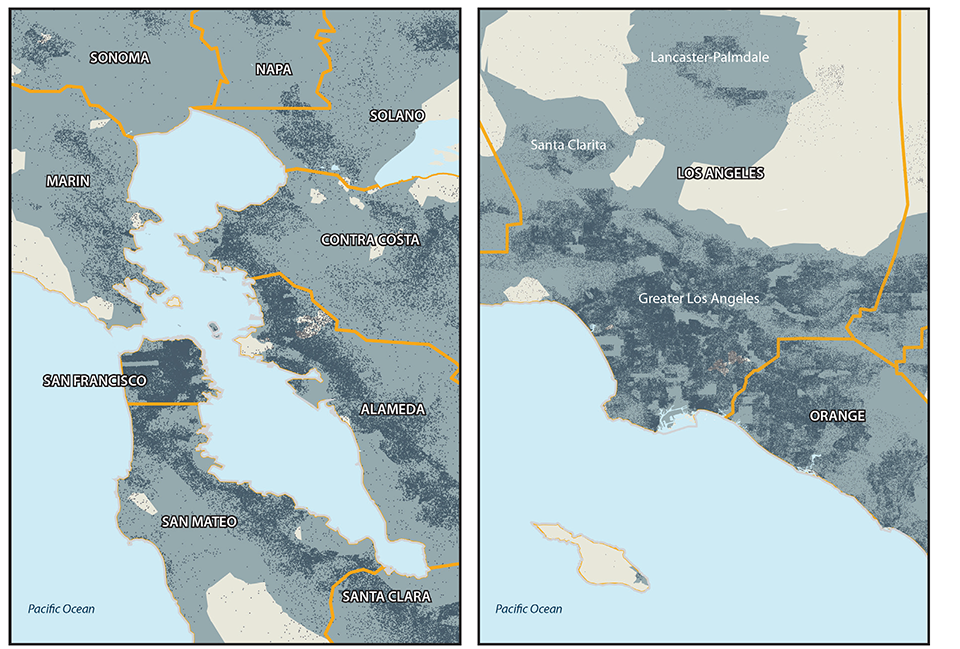
Although California has fewer free pharmaceutical collection sites than sharps collection sites, consumers generally have a similar level of access due to the sites’ locations. As Figure 7 shows, pharmaceutical collection sites are generally spread throughout the State’s major population centers. This wide distribution of the sites in major population centers means that more than 34.6 million people, or 91 percent of the State’s population, have reasonable access. For example, the vast majority of Los Angeles County residents live within a 20‑minute drive of pharmaceutical collection sites. Similarly, as Figure 8 shows, most Bay Area residents also have reasonable access: most people residing in San Francisco, Alameda, and San Mateo counties need to drive 20 minutes or less to reach collection sites.
Click here for a closer look at Figure 7.
Figure 7
State and Federal Agencies Suggest Ways to Dispose of Home‑Generated Sharps and Pharmaceutical Waste
Source: California State Auditor’s analysis of federal and state agencies’ messages about proper disposal of home‑generated sharps and pharmaceutical waste.
We estimate that 3.4 million people may live farther than a 20‑minute drive from pharmaceutical waste collection sites, particularly in the State’s areas of low population density and in less populous urban areas. For instance, Figure 8 shows that Imperial County—despite having several urbanized areas and a population greater than 177,000—does not contain any pharmaceutical collection sites that we identified in our analysis. However, our sources, and therefore our analysis, did not differentiate consistently between those pharmaceutical waste collection sites that do and do not accept controlled substances.
Figure 8
State and Federal Agencies Suggest Ways to Dispose of Home‑Generated Sharps and Pharmaceutical Waste

Source: California State Auditor’s analysis of federal and state agencies’ messages about proper disposal of home‑generated sharps and pharmaceutical waste.
The State Does Not Provide Reliable Information to Ensure That Consumers Are Aware of Available Collection Sites
Although the majority of residents have reasonable access to sharps and pharmaceutical waste collection sites, public information regarding those sites is scattered, inconsistent, and sometimes inaccurate. No state agency is responsible for maintaining an accurate, complete, and up‑to‑date list of sharps and pharmaceutical collection sites. Nonetheless, while not required to do so, two agencies—Public Health and CalRecycle—publish on their websites lists they have compiled of statewide collection sites for both sharps and pharmaceutical waste. These agencies’ lists, however, have significant deficiencies that limit their usefulness.
CalRecycle also maintains a list of sharps and pharmaceutical collection sites as part of its Facility Information Toolbox (FacIT) database, which identifies solid waste and recycling facilities across the State. However, CalRecycle cautioned that it did not design FacIT to track sharps and pharmaceutical collection sites but rather to serve as an inventory of all California waste and recycling facilities for its own planning and policy purposes. We found errors in this list too, such as facilities that had closed. Further, one of CalRecycle’s sources of information for FacIT is the list of sites that Public Health has collected, which as noted above contained errors. Consequently, consumers who rely on either Public Health or CalRecycle for the locations of pharmaceutical and sharps collection sites may not obtain up‑to‑date or reliable information.
In addition to problems with the completeness and accuracy of the information they offer, neither Public Health nor CalRecycle makes their lists readily accessible and user‑friendly. Public Health’s list of sharps and pharmaceutical collection sites contains detailed information on collection site practices. However, the format in which Public Health presents its list is awkward for consumers to use because the entries for disposal sites are difficult to read. Further, consumers cannot sort the list for relevant information, such as disposal sites’ locations by city or county and the types of waste that the sites collect. On the other hand, CalRecycle’s FacIT database has users navigate a detailed set of drop‑down menus, which are more user‑friendly than Public Health’s list but require users to choose among many potentially confusing options. Finally, neither agency’s list is readily designed for use on mobile devices.
State agencies could make their lists more accessible by modeling them on a website that several local agencies in the San Francisco Bay Area created. This website, Recyclewhere.org, is a collaboration between the San Francisco Department of the Environment, the Alameda County Waste Management Authority, Contra Costa County, and the cities of San Jose and Palo Alto. According to the website, its goal is to reduce many types of waste—not just sharps and pharmaceuticals—by providing accurate information about recycling, reuse, and proper disposal options for residents and businesses without regard to traditional municipal boundaries. The website’s search interface allows users to enter the types of waste they are trying to dispose of and their zip codes. The website then delivers locations to the users based on their zip codes. The website also works well on mobile platforms, increasing its accessibility. A similar format would significantly improve the lists that Public Health and CalRecycle currently provide. If consumers can easily access accurate, searchable information about collection sites for sharps and pharmaceutical waste, they might be more likely to dispose of these products properly.
The State Could Implement Alternative Disposal Methods in Rural Areas
As we previously note, four million Californians may lack reasonable access to collection sites. Establishing more collection sites in rural areas may not be practical, given that the cost of hiring hazardous waste or medical waste haulers to collect waste from remote collection sites may be prohibitive. However, the State could implement alternate disposal methods for consumers who lack access to collection sites. For example, the State could subsidize these consumers’ use of mail‑back containers or envelopes to dispose of home‑generated sharps and pharmaceutical waste. Consumers can fill the containers—which come in various sizes and can safely contain sharps or pharmaceutical waste—and mail them for disposal via DEA‑registered mail‑back collectors. Federal and state agencies—including the EPA, DEA, FDA, CalRecycle, and Public Health—promote mail‑back systems as safe disposal methods for sharps and pharmaceutical waste.
Although mail‑back options can be expensive on a small scale, they may be the most cost‑effective option for rural areas. According to retail websites, the cost for a prepaid mail‑back container is often $30 or more. However, the State might be able to use its buying power to purchase these containers in bulk at lower prices than might be available to individuals. The University of Maine ran a pilot mail‑back program between 2008 and 2012 that provided Maine residents with free prepaid mail‑back envelopes for disposing of their unwanted medications. The program began with funding from the EPA, and it shifted to state funding eventually to extend the program’s duration by two years. In a report it published on the program, the University of Maine concluded that mail‑back programs were both feasible and effective. It noted that the program had diverted a large amount of pharmaceutical waste from the water system and landfills. If California were to provide rural residents with free or subsidized mail‑back containers for their sharps and pharmaceutical waste, the State could encourage proper disposal without incurring the costs of maintaining permanent collection sites in areas with low‑population densities.
The State Lacks Data on the Volume of Sharps and Pharmaceutical Waste That Consumers Generate and the Ways in Which They Dispose of This Waste
For this audit, the Legislature asked us to estimate the volume of sharps and pharmaceutical waste that consumers properly discarded over the past three years. However, accurately estimating this amount is challenging for a number of reasons. Specifically, no state agency currently attempts to collect comprehensive and reliable data on the amount of home‑generated sharps and pharmaceutical waste that consumers properly dispose of in California. Further, even if a state agency were charged with this responsibility, collecting accurate and comprehensive information would present significant challenges because of the data sources involved. CalRecycle is the only state agency that collects any data on home‑generated sharps and pharmaceutical waste, but it only collects data from hazardous waste sites and does not verify the data’s accuracy or completeness. The three local governments we visited also collect limited data, but there is no requirement that they report to any state agencies any information beyond their data for household hazardous waste sites. In addition, state law does not require California’s 37 locally authorized syringe exchange programs to track the number of sharps they distribute and collect and this omission creates an additional gap in monitoring home‑generated sharps and pharmaceutical waste.
Public Health, Toxic Substances Control, and the Pharmacy Board all stated that they do not collect or maintain data on amounts of home‑generated sharps and pharmaceutical waste. Although state regulation requires local agencies that are responsible for household hazardous waste sites to report the amounts of waste they collect through CalRecycle’s reporting database, the resulting data are neither accurate nor complete. CalRecycle does not validate the amounts of waste the household hazardous waste sites report, nor does it take any actions when sites fail to report collection data because it asserts that state law does not give it funding to enforce this reporting. Not surprisingly, our review found that CalRecycle’s data had numerous errors, including repeat entries, obvious gaps in reporting, and potentially inconsistent measurements of the volume of sharps and pharmaceuticals. As a result of these problems, CalRecycle’s database is not a reliable source of information for the volume of home‑generated sharps and pharmaceutical waste.
Moreover, even if CalRecycle’s database contained accurate and complete information, the State would still lack reliable data from other entities that collect sharps and pharmaceutical waste. The existing data we identified have significant limitations and are either insufficient or inappropriate for reasonably estimating the amount of home‑generated sharps and pharmaceutical waste consumers properly dispose of in California. Some of the programs that have collected this existing data include pharmaceutical disposal sites, mail‑back programs, and syringe exchanges. For example, the California Product Stewardship Council, an advocacy group, asserts that it collected nearly 5,400 pounds of unwanted medications between July 2013 and December 2015. However, it did not track or retain support for this assertion.
Similarly, most syringe exchange programs either do not collect data on waste or do not ensure the accuracy of the data they do collect. The primary mission of most locally authorized syringe exchange programs is to ensure access to clean needles and to reduce the transmission of diseases such as HIV and hepatitis among people who inject drugs. Syringe exchange programs also provide a method for program participants to dispose of used sharps in a safe manner. Nonetheless, state law does not require locally authorized programs to collect data regarding the numbers of sharps they distribute and collect. Our review of programs in the counties we visited—San Luis Obispo, Orange, and San Francisco—indicated that these programs’ data are often unreliable and have significant limitations. For example, the local agencies that oversee these syringe exchange programs often do not validate the data the programs collect. Further, although state law requires local health officers to report biennially in open meetings of county boards of supervisors or city councils about local agencies’ syringe exchange program activities, it does not require this reporting to include the numbers of syringes that the programs collect or distribute.
Because of the limitations of the available data sources, accurately estimating the volume of sharps and pharmaceutical waste that consumers dispose of properly is challenging. However, in an attempt to respond to the Legislature’s audit request, we used the best available data to make rough estimates. As Table 3 shows, we based our estimates on many sources of varying levels of reliability, none of which we consider fully reliable. Because we were unable to determine the accuracy and completeness of these data sources, our estimates should not be used to guide policy decisions. Further, this estimate does not provide the information that might be most useful to decision makers: the amounts of these types of waste that consumers dispose of improperly. Collecting such data is probably impossible because consumers may improperly dispose of sharps and pharmaceutical waste in the sewer or trash.
Using local data from San Francisco’s programs and the available statewide data, we estimated that entities statewide collect 900,000 pounds of pharmaceutical waste and 2.8 million pounds of sharps waste annually. We used San Francisco’s data to generate statewide estimates of the volume of properly discarded home‑generated sharps and pharmaceutical waste because San Francisco’s large population makes its data less variable than that of cities or counties with smaller populations. In addition, San Francisco had more sources of data than the other two counties we visited. San Francisco’s pilot program for pharmaceutical collection, the Safe Needle Disposal Program, and its household hazardous waste sites all had data available. However, our estimate for pharmaceutical waste may be high because San Francisco has a robust pharmaceutical disposal program that offers residents the opportunity to dispose of expired or unwanted medicines at 13 independent pharmacies and at all 10 of San Francisco’s police stations.
Finally, we note that even if it were possible to determine the amounts of sharps and pharmaceutical waste that consumers dispose of properly, the State would still have no way of knowing the amounts of these types of waste that consumers dispose of improperly. No agency can measure accurately the amount of improperly discarded sharps and pharmaceuticals because some consumers flush their waste or throw it in the trash. CalRecycle’s 2015 Waste Characterization Study attempted to quantify the types and amounts of waste generated in the State. However, it did not identify sharps and pharmaceutical waste specifically. Therefore, this study could not be used in developing estimates of the amounts of improperly disposed of sharps and pharmaceutical waste.
| PHARMACEUTICAL waste | Data from San Francisco Sources | Statewide Multiplier* | Total (In Pounds) | ||||
|---|---|---|---|---|---|---|---|
| San Francisco’s pharmaceutical collection program, fiscal year 2015–16 | 18,000 | x36 | 648,000 | ||||
| DEA Prescription Take‑Back Day, statewide, 2016 | 64,000 | ||||||
| Household hazardous waste sites, statewide, fiscal year 2015–16 | 168,000 | ||||||
| Estimated pounds of properly disposed of pharmaceutical waste, annually, statewide | 880,000 | ||||||
| SHARPS Waste | Data From San Francisco Sources | Statewide Multiplier | Total (In Pounds) | ||||
| San Francisco Safe Needle Disposal Program, fiscal year 2015–16 | 30,000 | x36 | 1,080,000 | ||||
| Household hazardous waste sites, statewide, fiscal year 2015–16 Sharps waste from San Francisco’s syringe exchange programs | 567,000 | ||||||
| July–September 2016 | 772,000 x 4 |
||||||
| Multiplied by 4 for an annual estimate | 3,088,000 | ||||||
| Divide by 100 because 100 syringes weigh about one pound.† | 3,088,000 ÷ 100 |
31,000 | x36 | 1,116,000 | |||
| Estimated pounds of properly discarded sharps waste each year, statewide | 2,763,000 |
Note: We highlight our level of confidence in each data source as follows:
Yellow = Moderate
Orange = Poor
Red = Very poor
* San Francisco’s 400,000 households account for about 1/36 of the 14 million households statewide.
† Unit size for sharps waste varies greatly, so we based our estimate of syringes‑per‑pound on a commonly used brand for injecting insulin.
California Has Sufficient Capacity for Processing Sharps Waste, but It Primarily Relies on Out‑of‑State Incinerators for Pharmaceutical Waste
California’s total collection amounts for sharps and pharmaceutical waste make up a negligible fraction of the available capacity of in‑state treatment sites. Consequently, collection programs for home‑generated sharps waste in the counties we visited mainly send sharps waste to in‑state medical waste treatment facilities that sterilize and dispose of that waste. However, because of federal and state regulations and recommendations related to the treatment of hazardous waste, collection sites send pharmaceutical waste to out‑of‑state incinerators. If California law specifically excluded household pharmaceutical waste from the definition of hazardous waste that applies to municipal solid waste incinerators, existing in‑state incinerators might accept more pharmaceutical waste, relieving collection sites of the burden of shipping waste out of state for destruction.
Most Collection Sites Dispose of Sharps Waste in the State but Ship Pharmaceutical Waste to Out‑of‑State Incinerators
California law requires collection sites to treat consolidated home‑generated sharps waste as medical waste, meaning that only approved medical waste treatment facilities can process it. These facilities primarily use autoclaving—a steam sterilization process involving pressure and heat—to process the sharps before disposing of them in landfills as solid waste. California has 18 medical waste treatment facilities, 16 of which use the autoclaving process.
However, if household hazardous waste sites mix home‑generated sharps with other hazardous waste, these sites must treat that composite waste as hazardous rather than as medical waste. State law imposes additional requirements on the processing of hazardous waste. If sites process sharps as hazardous waste using incineration, they must send the waste out of state because there are no commercial hazardous waste incinerators within California. This situation is due in part to onerous permitting requirements and public opposition to hazardous waste incinerators. For example, Orange County collects sharps at its household hazardous waste sites, then contracts with a hazardous waste hauler to ship the sharps to out‑of‑state facilities for incineration.
Similarly, collection sites often send pharmaceutical waste out of state for incineration. These practices may be occurring because the model guidelines that CalRecycle outlined in its 2010 report, which we discuss in the Introduction, recommend collectors manage consolidated home‑generated pharmaceutical waste as medical or hazardous waste. Furthermore, the EPA recommended in 2012 that collection sites destroy household pharmaceutical waste at hazardous waste incinerators, or, if these prove cost‑prohibitive, at solid waste incinerators.
When collection programs treat pharmaceutical waste as medical or hazardous waste, they contract with waste haulers who mainly transfer the waste to incinerators in other states. Just as it lacks hazardous waste incinerators, California does not have any commercial medical waste incinerators because regulators at the state level place legal restrictions on these incinerators. For instance, the California Air Resources Board limits the amounts of dioxin emissions medical incinerators can produce. Consequently, two of the counties we visited transport pharmaceutical waste out of state for incineration. For example, San Francisco contracts with a medical waste hauler to transport out of state the waste that pharmacies collect through its pilot program for pharmaceutical collection.
In addition, if pharmaceutical waste includes controlled substances, the DEA requires collection sites to ensure that such waste is rendered irretrievable, and this process usually means some form of incineration. Although the DEA does not require that controlled substances be destroyed using a specific method, the only entities allowed to collect controlled substances for disposal are law enforcement or DEA‑registered collectors, such as retail pharmacies. Because California’s solid waste incinerators are not registered with the DEA, they can only destroy controlled substances under the direct supervision of DEA registrants or law enforcement personnel.
Both In‑State and Out‑of‑State Facilities Have Sufficient Capacity to Process Significant Increases in California’s Sharps or Pharmaceutical Waste
As previously mentioned, California has 18 medical waste treatment sites that can process sharps. According to facility permit applications held at Public Health, these medical waste treatment facilities have available capacity—beyond what they currently process—of 288 million pounds per year. Also discussed earlier, we estimate that California may currently collect as much as 2.8 million pounds of home‑generated sharps per year, an amount that is about 1 percent of the available capacity at medical waste treatment facilities. Thus, the existing in‑state capacity for medical waste treatment is more than sufficient to process significant increases in the State’s home‑generated sharps waste.
Similarly, hazardous waste incinerators outside of California have sufficient capacity to process future increases in the State’s sharps waste. According to the EPA, eight commercial incinerators for hazardous waste operated in the United States in 2014. These incinerators have a combined available capacity—beyond what they currently process—to handle about 800 million pounds of home‑generated sharps per year. The EPA predicts this available incineration capacity will remain stable through 2039. Thus, the eight commercial hazardous waste incinerators have more than sufficient available capacity to process any conceivable increase in sharps waste that California ships out of state.
Out‑of‑state incineration capacity is also sufficient to meet California’s pharmaceutical disposal needs. Our estimates suggest that California may collect as much as 900,000 pounds of pharmaceutical waste per year. With 800 million pounds of available capacity annually, the eight out‑of‑state incinerators have ample capacity to destroy that waste. Additionally, the EPA estimates that the 10 out‑of‑state commercial incinerators for medical waste that were operating in 2013 had an annual available capacity of at least 110 million pounds. Thus, their capacity is also more than sufficient to process all of California’s estimated 900,000 pounds of pharmaceutical waste per year should the State choose to process it as medical waste.
Exempting Pharmaceutical Waste From the State’s Definition of Hazardous Waste Would Allow for More In‑State Incineration
Despite the fact that California currently sends most of its home‑generated pharmaceutical waste out of state for incineration, the State has the available capacity to incinerate it in state. Specifically, California has three active waste‑to‑energy incinerators for solid waste: two in Los Angeles County and one in Stanislaus County. All three California incinerators have processed home‑generated pharmaceutical waste in the past or explicitly allow it in their operations documents under certain circumstances, such as when law enforcement needs to destroy controlled substances.
However, despite having the available capacity, there are barriers to incinerating pharmaceutical waste in California. Specifically, California law does not exclude home‑generated pharmaceutical waste from the legal definition of hazardous waste that applies to solid waste incinerators. Moreover, the law requires their permits to contain procedures that prevent hazardous waste from entering the incineration process. Consequently, the operators of these in‑state incinerators may put their permits at risk if they accept pharmaceutical waste.
The State could relieve collection sites of the burden of shipping home‑generated pharmaceutical waste out of state for destruction by specifically excluding it from the definition of hazardous waste. If California law were to exempt home‑generated pharmaceutical waste from its definition of hazardous waste for municipal waste incinerators, then these existing in‑state incinerators might accept more pharmaceutical waste. The three California’s waste‑to‑energy incinerators for solid waste have available capacity of more than 600 million pounds per year. That capacity is much greater than the State’s total pharmaceutical waste collection. Thus, California’s incinerators have the capacity to process all nonhazardous, noncontrolled pharmaceutical waste that collection sites currently transport out of state.
Processing more pharmaceutical waste in state could result in savings for collection sites. According to sources we consulted, distance is a factor in medical waste disposal pricing. The farther the haulers must transport waste, the greater the cost. California’s pharmaceutical waste is often shipped to other states for disposal: for instance, a contractor ships San Luis Obispo’s pharmaceutical waste to Maryland, North Carolina, and Texas for destruction. Destroying such waste in state could thus create cost savings for community collection sites. In Florida, for example, in‑state municipal waste combustors are allowed to incinerate or burn limited quantities of pharmaceutical waste. The Florida Department of Environmental Protection concluded that the expected impact on emissions of incinerating more pharmaceutical waste in state would be negligible—and probably undetectable.
Other States and Countries Follow Collection and Disposal Practices That Could Serve as Models for California
California could benefit by adopting some aspects of programs that other governments have implemented for disposal of home‑generated sharps and pharmaceutical waste. Although other governments’ programs may address different goals and target different geographic locations, one of their primary purposes is to reduce health risks associated with the disposal of sharps and pharmaceutical waste. However, comparing the performance of the programs is difficult because most of the programs do not collect data consistently, if at all. In addition, CalRecycle has outlined several model program options for pharmaceutical waste collection that California could adopt, but it is unclear who would bear the costs for those programs.
California Could Employ Elements of Programs From Other States and Countries
Other states and countries have developed and implemented a number of home‑generated sharps and pharmaceutical waste disposal programs that could potentially influence California in a positive way. Some programs we identified focus on consumer education. For example, the state of New York (New York) requires all pharmacies and other retail businesses that sell pharmaceuticals to prominently display New York’s approved pharmaceutical disposal methods. This law facilitates a public information campaign called Don’t Flush that educates consumers on the proper disposal of home‑generated pharmaceutical waste. However, New York does not collect or track data related to this campaign. Sweden also employed a month‑long education campaign in 2012 to encourage consumers to dispose of their unused medications at pharmacies. After the campaign, Sweden reported that the return of unwanted medications increased 6 percent from the previous year.
Similarly, Canada has two nationwide programs that focus on raising public awareness of the benefits of proper disposal of pharmaceutical waste. Specifically, Canada uses a pharmaceutical drop‑off day modeled after the U.S. National Prescription Drug Take‑Back Day. In addition, a private nonprofit manages an annual, six‑month‑long prescription take‑back campaign that encourages Canadians to dispose of expired drugs at any of the participating pharmacies throughout the country. This campaign aims to keep medications out of the hands of young people and promotes awareness and best practices for medication use and disposal.
In addition, several Canadian provinces have implemented extended producer responsibility programs (EPR programs) for sharps and pharmaceutical waste. EPR programs assign to the products’ producers or manufacturers the costs, and often the design, of the disposal plans for those products. Four Canadian provinces have adopted provincewide programs for sharps collection, two of which use the EPR program model, while seven Canadian provinces have adopted provincewide programs for pharmaceutical collection, six of which use the EPR program model. Although Canada lacks accessible data on the volume of home‑generated sharps and pharmaceutical waste the country as a whole collects, some of its province‑level programs publish limited data on their efforts. For example, the sharps and pharmaceutical industry runs an EPR program in the province of Ontario. The program indicated in its annual report for 2016 that its collection of sharps waste had increased by 19 percent and that its collection of pharmaceutical waste had increased by 16 percent since 2015. Using these data, the executive director of the program concluded that Ontario’s program was effective and efficient and that consumer awareness of it was increasing.
Unfortunately, even though the Canadian government reports some data on program collection amounts, it does not report sufficient data to compare different programs’ effectiveness. For example, although Canada used as measures the sizes of containers filled when reporting Prince Edward Island’s pharmaceutical collections, it used the weights of pharmaceutical waste when reporting Manitoba’s collections. Thus, we could not compare the outcomes of these two programs.
As we show in Table 4, the disposal and collection programs we identified have different policy goals that reflect the collection and disposal needs of the states or countries that implemented them. For example, Minnesota created its Take It to the Box pharmaceutical collection and disposal campaign to reduce the risks of accidental poisoning, theft, and drug abuse, while Sweden developed its education campaign for pharmaceutical waste to reduce the environmental impact of discarded medications. Before California can implement a new collection program for home‑generated sharps and pharmaceuticals, the Legislature and the responsible state oversight agency will need to identify policy goals for the program and ensure that those goals align with state and federal laws.
| Goal | Location | Program | Program Purpose | Funding Source | |
|---|---|---|---|---|---|
| SHARPS WASTE | |||||
| 1 | Health, Safety, and Environment | New York | Safe Sharps Collection Program | Legally requires all hospitals and nursing homes in the state to collect household sharps. | State |
| 2 | Health | New York | Syringe Exchange Program | Provides sterile syringes and collects used syringes from program participants. | State |
| 3 | Health | Maine | Syringe Exchange Program | Provides sterile syringes and collects used syringes from injection drug users. | Private |
| 4 | Health | Sweden | Syringe Exchange Program | Provides sterile syringes and collects used syringes from injection drug users. | Local government |
| 5 | Health | New York | Expanded Syringe Access Program | Allows pharmacies to sell syringes without a prescription to anyone over the age of 18. | State |
| 6 | Health | Minnesota | Syringe/Needle Access Initiative | Allows pharmacies to sell syringes to customers without prescriptions. | None needed |
| 7 | Education | Maine | Safe Sharps Disposal | Distributes 40,000 brochures regarding the safe disposal of household sharps and provides 3,000 free needle‑clipping devices. | Private |
| 8 | Safety | France | DASTRI Program | Requires pharmacies to provide sharps containers to consumers, who can dispose of them at collection sites throughout the country. | Private |
| PHARMACEUTICAL WASTE | |||||
| 1 | Environment | New York | Don’t Flush Your Drugs | Requires all pharmacies and retailers that sell pharmaceuticals to display a poster outlining proper disposal methods. | None Needed |
| 2 | Health, Safety, Environment | Minnesota | Take It to the Box | Provides, through its Pollution Control Agency, free informational materials to local agencies and installs in their jurisdictions drop boxes for pharmaceutical waste. | Private |
| 3 | Safety | Canada | National Medicine Take‑Back Campaign | Establishes an annual take‑back campaign where pharmacies nationwide collect pharmaceutical waste from July through December. | Private |
| 4 | Health, Safety, Education | Spain | SIGRE Program | Ensures an industry‑managed collection and disposal program. | Private |
| 5 | Education | Maine | Safe Medicine Disposal for ME | Provide participants with free prepaid mail‑back envelopes. | Federal and State |
| 6 | Environment and Education | Sweden | Apoteket AB | Educates and encourages consumers to dispose of their unused medications at pharmacies. | Unknown |
| 7 | Environment and Health | France | Cyclamed | Allows pharmaceutical waste disposal at all pharmacies in France. | Private |
In 2010 CalRecycle Provided the State With Options for Pharmaceutical Waste Collection Programs
In 2007 the Legislature passed Senate Bill 966 (SB 966) requiring CalRecycle to develop and report on recommendations for model pharmaceutical waste collection programs in the State. The bill identified minimum criteria the programs must meet, including the safe and environmentally sound collection and disposal of unused or expired home‑generated pharmaceuticals at no additional cost to the consumers. It also required the model programs to include informational materials for consumers about opportunities for the proper disposal of pharmaceutical waste and the potential impacts of improper disposal. Further, SB 966 required CalRecycle to consult federal, state, and local agencies in developing model guidelines for the collection and proper disposal of pharmaceutical waste.
In response to the bill, CalRecycle submitted to the Legislature its report, Recommendations for Home‑Generated Pharmaceutical Collection Programs in California (recommendations report), in December 2010. CalRecycle provided the Legislature four different model program options to consider. The first option involves leaving the current system in place while emphasizing the importance of following the model guidelines CalRecycle developed in response to SB 966. The second option entails clearly establishing state agencies’ roles and responsibilities related to pharmaceutical waste collection, including providing an agency with enforcement authority; further, this option involves converting the model guidelines into regulations. The third option is the implementation of a statewide EPR program that—as discussed previously—would place the responsibility and costs for collecting and disposing of waste on the products’ manufacturers. Finally, the fourth option is an advance disposal fee program, which would require consumers to pay a fee at the time of purchase to finance a state‑managed program to collect pharmaceutical waste.
Our review of these recommended model program options suggests that the second may be the most feasible. Specifically, we believe that the first option would not result in significant change to the State’s current system, which has a number of weaknesses, as we discuss in this report. Further, as Table 5 shows, either implementing a statewide EPR program or using an advanced disposal fee program would likely result in passing disposal costs onto consumers, a situation inconsistent with the criteria the Legislature established for model programs. The second option, therefore, is the only program that would address weaknesses in the current system without creating additional costs for consumers. A key element of this option is the identification of a state agency to develop regulations that would make CalRecycle’s model guidelines mandatory. This recommendation assumes that individual collection programs would not receive additional funding but acknowledges that the designated state agency would require additional resources to develop and implement regulations. As this report discussed previously, we believe that the Legislature should designate CalRecycle as the lead agency.
| Option | Recommended Program | Does this program represent change? | Would this program Require a lead state agency? | Who would manage this program? | Who would absorb costs? |
|---|---|---|---|---|---|
| 1 | Continue current use of model guidelines: the State would maintain the voluntary model guidelines and encourage consumers to follow federal guidelines. | No | No | Unclear | State agency and local governments |
| 2 | Establish clear state agency roles and responsibilities, improve model guidelines and enforcement, and convert guidelines to regulations. This option provides a state agency with authority to enforce the model guidelines. | Yes | Yes | Lead state agency and local governments | Lead state agency and local agencies |
| 3 | Implement an EPR program with private sector leadership: pharmaceutical manufacturers would design, manage, and finance a statewide program, while state government would oversee program implementation and enforcement. | Yes | Yes | Pharmaceutical producers and stewardship organizations with some state oversight | Consumers |
| 4 | Create a state collection program using an advance disposal fee and state oversight: this option would require consumers to pay a fee at the time they purchase sharps, medications, or medical devices. Funds would finance the collection program. | Yes | Yes | CalRecycle or other state agency | CalRecycle or other state agency and consumers |
However, CalRecycle’s recommendations report ultimately proposes a combination of converting the model guidelines into regulations, making statutory changes to establish clear state agency roles and responsibilities, and developing a statewide program for disposing of home‑generated pharmaceutical waste based on an EPR program model. The California Product Stewardship Council and other entities support the implementation of EPR programs by highlighting the risks of improper disposal of sharps and pharmaceutical waste. Additionally, the California Product Stewardship Council supports policies and projects in which producers share in the responsibility for managing problem products at the end of the products’ lives. Similar programs already exist in California for carpet, mattresses, and paint. Nonetheless, developing a statewide EPR program would present several challenges, which CalRecycle acknowledged. For example, although the EPR program model requires manufacturers to fund collection programs, manufacturers are likely to pass on those costs to consumers, either directly or indirectly. In addition, the implementation of a statewide EPR program would require new legislation, which CalRecycle believed would be difficult to enact. Overcoming these challenges would be necessary for making a statewide EPR program successful.
Moreover, sharps and pharmaceutical manufacturers are resistant to the implementation of a statewide EPR program. For example, the representatives with whom we spoke believe that it would be inappropriate for the sharps and pharmaceutical industry to bear the costs to dispose of sharps waste from illegal drug users. One company’s representative stated that it already manages a free take‑back program for its own syringes by including mail‑back envelopes with its product. Further, industry representatives indicate that EPR programs place an additional cost burden on consumers and that they potentially erect market barriers for companies seeking to sell sharps products in California. Industry representatives also assert that various studies show there is minimal health risk due to improper disposal of home‑generated sharps waste in consumer trash and that pharmaceutical take‑back programs do not result in improved water quality. They stated that the existing problems are the result of failings in the current system for disposing of home‑generated sharps and pharmaceutical waste. For example, they noted that there is insufficient education and outreach to consumers on the methods to properly dispose of sharps and pharmaceutical waste.
However, industry representatives indicated that they would prefer the establishment of uniform EPR program requirements across the State to their companies’ meeting requirements that differ by county, as they currently must. Some California counties, including San Francisco and Alameda, have already adopted local EPR program ordinances. Trade associations representing manufacturers and distributors of pharmaceuticals challenged implementation of the ordinance in Alameda by arguing that it interfered with interstate commerce. Nonetheless, federal courts upheld Alameda’s ordinance. According to the representatives with whom we spoke, implementing EPR programs on a county‑by‑county level creates inefficiencies for pharmaceutical manufacturers because each county may establish different requirements, and inconsistencies among local programs can confuse consumers. Further, the representatives indicate that implementation of various local ordinances forestalls conversations at the state and national levels around effective and equitable solutions
The counties that have already established EPR ordinances have faced additional challenges as well. For example, according to Alameda, the first county to implement a pharmaceutical EPR program in California, a significant barrier towards full implementation of its EPR program is reaching agreement with pharmacies to serve as collection sites. Pharmacies are logical locations to serve as pharmaceutical waste collection sites because consumers can properly dispose of unused medications when filling new prescriptions. However, Alameda’s pharmaceutical waste ordinance makes pharmacies’ participation voluntary, and Alameda indicates that major pharmacy chains have not yet participated.
As previously discussed, we recommend that the Legislature implement the second option that CalRecycle’s recommendations report proposes and that the Legislature identify CalRecycle as the lead agency for ensuring the proper disposal of sharps and pharmaceutical waste. The Legislature could also establish an alternative to a statewide EPR program that would better enable counties to implement their own EPR programs if they desire to do so. Specifically, the Legislature could establish guidelines for counties that choose to implement their own EPR programs. Such guidelines would incorporate the Legislature’s policy decisions and provide consistency among counties’ EPR programs, while limiting the costs that could get passed on to consumers. For example, the guidelines could address whether the counties’ EPR programs would include the collection of nonprescription medications and whether they should provide a mail‑back component. This increased consistency would allow manufacturers to comply more readily with EPR programs in California.
Recommendations
- Developing and implementing a public education campaign about home‑generated sharps and pharmaceutical waste disposal. CalRecycle should coordinate this campaign with local, state, and, to the extent possible, federal agencies to ensure consumers receive consistent guidance regarding proper disposal methods.
- Maintaining an up‑to‑date, well‑publicized, and accessible statewide list of free sharps and pharmaceutical waste collection sites. CalRecycle should create this list by either improving its FacIT database or by establishing a new database, potentially using Recyclewhere.org as a model.
- Increasing consumers’ access to proper disposal methods in underserved locations. It could increase access by subsidizing prepaid mail‑back options or by encouraging municipalities to include the collection of sharps and pharmaceutical waste in their contracts with waste haulers.
- Determining the characteristics of other government programs, such as New York State’s consumer education program, that might benefit California.
To increase in‑state options for processing California’s home‑generated pharmaceutical waste, the Legislature should expressly authorize municipal solid waste incinerators to burn limited quantities of home‑generated pharmaceutical waste, but only after considering environmental impacts.
We conducted this audit under the authority vested in the California State Auditor by Section 8543 et seq. of the California Government Code and according to generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives specified in the Scope and Methodology section of the report. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Respectfully submitted,
DOUG CORDINER, CGFM
Chief Deputy State Auditor
Date:
May 9, 2017
Staff:
John Baier, CPA, Audit Principal
Josh Hooper, CIA, CFE
Sharon L. Fuller, CPA
Katie Cardenas, MPPA
Brianna J. Carlson
Joseph Miller
Lisa J. Sophie, MPH
Legal Counsel:
Joseph L. Porche, Staff Counsel
For questions regarding the contents of this report, please contact Margarita Fernández, Chief of Public Affairs, at 916.445.0255.
Footnotes
1 Our Appendix provides information on access using different driving times to sharps and pharmaceutical waste collection sites.
Go back to textBack to top