
San Diego County Sheriff’s Department
It Has Failed to Adequately Prevent and Respond to the Deaths of Individuals in Its Custody
February 3, 2022
2021-109
The Governor of California
President pro Tempore of the Senate
Speaker of the Assembly
State Capitol
Sacramento, California 95814
Dear Governor and Legislative Leaders:
As directed by the Joint Legislative Audit Committee, my office conducted an audit of the San Diego County Sheriff’s Department (Sheriff’s Department) to determine the reasons for in‑custody deaths of incarcerated individuals and identify the steps it took to address these deaths. The following report details our conclusion that the Sheriff’s Department has failed to adequately prevent and respond to the deaths of individuals in its custody.
From 2006 through 2020, 185 people died in San Diego County’s jails—one of the highest totals among counties in the State. The high rate of deaths in San Diego County’s jails compared to other counties raises concerns about underlying systemic issues with the Sheriff’s Department’s policies and practices. In fact, our review identified deficiencies with how the Sheriff’s Department provides care for and protects incarcerated individuals, which likely contributed to in‑custody deaths. These deficiencies related to its provision of medical and mental health care and its performance of visual checks to ensure the safety and health of individuals in its custody.
Furthermore, the Sheriff’s Department has not consistently taken meaningful action when such deaths have occurred. The department’s reviews of in‑custody deaths have been insufficient and have not consistently led to significant corrective action. In addition, the Citizens’ Law Enforcement Review Board (CLERB)—a citizen‑governed board approved by San Diego County voters to restore public confidence in county law enforcement—has failed to provide effective, independent oversight of in‑custody deaths. CLERB also failed to investigate nearly one‑third of the deaths of incarcerated individuals in the past 15 years, which means that dozens of deaths have not been subject to a key form of review outside of the Sheriff’s Department.
In light of the ongoing risk to inmate safety, the Sheriff’s Department’s inadequate response to deaths, and the lack of effective independent oversight, we believe that the Legislature must take action to ensure that the Sheriff’s Department implements meaningful changes.
Respectfully submitted,
MICHAEL S. TILDEN, CPA
Acting California State Auditor
Selected Abbreviations Used in This Report
| ADP | average daily population |
| BSCC | Board of State and Community Corrections |
| CDCR | California Department of Corrections and Rehabilitation |
| CLERB | Citizens’ Law Enforcement Review Board |
| POBR | Public Safety Officers Procedural Bill of Rights |
Summary
Audit Highlights . . .
Our audit of the San Diego County Sheriff’s Department’s response to deaths of individuals in its custody highlighted the following:
- » Until the Sheriff’s Department implements meaningful change to improve its provision of medical and mental health care in its detention facilities, it will continue to jeopardize the safety and lives of individuals in its custody.
• We found multiple instances of individuals who requested or required medical and mental health care and did not receive it at all or in a timely manner.
• In our review of deaths that occurred in the department’s custody, deputies performed inadequate safety checks to ensure the well‑being of those individuals. - » Some of the Sheriff’s Department’s policy deficiencies are the result of statewide corrections standards that are insufficient for maintaining the safety of incarcerated individuals.
• The Board of State and Community Corrections should require mental health evaluations to be performed by mental health professionals at intake, and it should clarify and improve procedures for safety checks. - » The entities responsible for investigating in‑custody deaths are not doing so in a thorough, timely, or transparent manner.
• The department’s Critical Incident Review Board should consistently review deaths by natural causes, increase public transparency, and take substantive steps to prevent similar future deaths.
• CLERB should prioritize the investigations of all deaths that occur in the department’s custody and complete those investigations within the one‑year statutory limit.
Results in Brief
In accordance with federal constitutional law, the San Diego County Sheriff’s Department (Sheriff’s Department) has a responsibility to provide adequate medical care for individuals while they are in its custody. Nonetheless, from 2006 through 2020, a total of 185 people died in San Diego County’s jails—more than in nearly any other county across the State. Some of these individuals were in custody for only a few days to a few months; others were waiting to be sentenced, set to be released, or about to be transferred to different facilities. Although any death is a tragedy, the high rate of deaths in San Diego County’s jails compared to other counties raises concerns and suggests that underlying systemic issues with the Sheriff’s Department’s policies and practices have undermined its ability to ensure the health and safety of the individuals in its custody.
Significant deficiencies in the Sheriff’s Department’s provision of care to incarcerated individuals likely contributed to the deaths in its jails. For example, studies on health care at correctional facilities have demonstrated that identifying individuals’ medical and mental health needs at intake—the initial screening process—is critical to ensuring their safety in custody. Nonetheless, our review of 30 individuals’ deaths from 2006 through 2020 found that some of these individuals had serious medical or mental health needs that the Sheriff’s Department’s health staff did not identify during the intake process. Some of these individuals died within four days of their arrest. Moreover, in one case we reviewed, an incident between two cellmates resulted in one’s death. In this instance, the intake nurse did not identify that the perpetrator had a history of mental health issues. Had the perpetrator’s mental health issues been identified properly at intake, the department’s staff might have placed this individual in a different cell, leading to a different outcome.
When we evaluated the intake practices of three comparable counties, we found that the counties had procedures that are more comprehensive. For example, the San Diego Sheriff’s Department relies on registered nurses to perform the mental health portion of its intake screening, even though these nurses may not specialize in mental health care. In contrast, the Riverside County Sheriff’s Department’s policy requires that a mental health clinician evaluate every individual at intake. Implementing similar policies could help the San Diego Sheriff’s Department to more effectively identify mental health needs early.
In addition, the Sheriff Department’s staff did not always provide consistent follow-up care to individuals who requested or previously received medical or mental health services. Best practices stress that timely treatment and follow‑up are important components of any health care system. Although the reasons that the Sheriff’s Department did not always follow up consistently—such as poor policies and communication—varied by case, they represent deficiencies in its medical and mental health care system that it needs to address.
For example, one individual urgently requested mental health services shortly after entering the jail. However, the nurse had not identified any significant mental health issues at intake and determined that the individual did not qualify for an immediate appointment. The individual died by suicide two days later—only four days after entering the jail. Although the Sheriff’s Department’s policy indicates that a face‑to‑face appraisal with an incarcerated individual should take place within 24 hours of a mental health care request to determine the urgency of that request, the department has not always had this policy. Further, this policy only applies to mental health requests and not medical health care requests. Thus, the Sheriff's Department does not ensure that it provides prompt care for all types of needs.
In addition to providing adequate health care, performing safety checks is a key component of ensuring the well‑being of individuals in detention facilities. Conducting these checks—which state law requires hourly through direct visual observation—is the Sheriff’s Department’s most consistent means of monitoring for medical distress and criminal activity. Nonetheless, in our review of 30 in‑custody deaths, we found instances in which deputies performed these checks inadequately. For example, based on our review of video recordings, we observed multiple instances in which staff spent no more than one second glancing into the individuals’ cells, sometimes without breaking stride, as they walked through the housing module. When staff members eventually checked more closely, they found that some of these individuals showed signs of having been dead for several hours. Although the Sheriff’s Department’s assistant sheriff of detentions indicated that the department has a process for periodically monitoring whether staff members adequately perform safety checks, it is not documented in policy. In contrast, the Riverside County Sheriff’s Department has a formal policy that requires supervising staff to regularly review videos of safety checks being performed, and it is thus in a better position to assess the quality of safety checks.
The problems we identified with the Sheriff’s Department’s policies are in part the result of statewide corrections standards that are not sufficiently robust. The Board of State and Community Corrections (BSCC) establishes in regulation the minimum standards that local detention facilities must follow. Every local jail system throughout the State uses these standards to create policies for inmate safety and care. However, some of the standards are insufficient for maintaining the safety of incarcerated individuals. For example, they do not explicitly require that mental health professionals perform the mental health screenings during the intake process. Further, they do not describe the actions that constitute an adequate safety check: rather, they simply state that safety checks must be conducted at least hourly through direct visual observation. Given that the annual number of incarcerated individuals’ deaths in county jails across the State increased from 130 in 2006 to 156 in 2020, improving the statewide standards is essential to ensuring the health and safety of individuals in custody in all counties.
In addition to its failure to adequately prevent the deaths of individuals in its custody, the Sheriff’s Department has not consistently taken meaningful action when such deaths have occurred. The department’s reviews of in‑custody deaths have been insufficient and have not consistently led to significant corrective action related to preventing deaths. The Sheriff’s Department’s internal entity for reviewing critical incidents, such as in‑custody deaths, and identifying corrective measures—the Critical Incident Review Board—has not always taken substantive steps to prevent similar future deaths in the cases we examined. The primary focus of this board is protecting the Sheriff’s Department against potential litigation rather than focusing on improving the health and welfare of incarcerated individuals. Further, this board generally does not review deaths from natural causes, which represented nearly half of the deaths of individuals in the custody of the Sheriff’s Department during the 15‑year period of our review. We are concerned that the Sheriff’s Department considers the Critical Incident Review Board’s reviews to be confidential under the attorney‑client privilege and does not have a process to report the results publicly. Consequently, the Sheriff’s Department risks conveying to the public that it is not taking these deaths seriously and making every effort possible to prevent similar deaths in the future.
The Sheriff’s Department has also not implemented certain key recommendations from external oversight entities. From 2006 through 2020, multiple external entities—including the San Diego County Grand Jury—have made recommendations to the Sheriff’s Department in areas related to inmate safety. Although the Sheriff’s Department implemented several of these recommendations, it did not take action on others, even though they were critical to improving the safety of individuals in its custody. For example, it did not implement recommendations that involved enhancing its safety checks and improving the way it communicates incarcerated individuals’ mental health needs to its staff.
To restore public confidence in county law enforcement, San Diego County voters approved the Citizens’ Law Enforcement Review Board (CLERB) in 1990, a citizen‑governed board. CLERB is responsible for reviewing complaints of misconduct and investigating deaths arising in connection with the actions of officers employed by the Sheriff’s Department or Probation Department. However, CLERB has failed to provide effective, independent oversight of in‑custody deaths. In violation of its own rules and regulations, CLERB’s investigations of the deaths of individuals in the Sheriff’s Department’s custody have not been independent, thorough, or timely. CLERB has not independently interviewed witnesses or visited the initial scenes of the deaths. Further, it has not consistently performed thorough investigations, and it relies largely on the reviews the Sheriff’s Department conducts.
Moreover, CLERB failed to review dozens of deaths in the Sheriff’s Department’s jails. State law generally requires that CLERB’s investigations be performed within a year of discovery of the death or misconduct. Because CLERB did not consistently prioritize its investigations of deaths over other complaints of misconduct, it did not review 13 cases involving deaths in the Sheriff’s Department’s jails within the required time limit. Further, CLERB did not investigate an additional 40 deaths because it did not believe its rules and regulations required it to review natural deaths. As a result, it did not identify any weaknesses in the Sheriff’s Department’s policies or processes that may have contributed to these deaths nor develop any recommendations to address these weaknesses. Although CLERB currently reviews natural deaths, it lacks specific language in its rules and regulations requiring it to do so, thus raising concerns about whether its staff could exclude those reviews in the future.
Given the ongoing risk to the safety of incarcerated individuals, the Sheriff’s Department’s inadequate response to deaths, and the lack of effective independent oversight, we believe that the Legislature must take action to ensure that the Sheriff’s Department implements meaningful changes. Until the Sheriff’s Department makes such changes, the weaknesses in its policies and practices will continue to jeopardize the health and lives of the individuals in its custody.
Summary of Key Recommendations
Legislature
The Legislature should amend state law to require the Sheriff’s Department to revise its policies to align with best practices related to performing intake health evaluations (including requiring that mental health professionals perform mental health evaluations), providing follow‑up medical and mental health care, conducting safety checks, and addressing the other deficiencies that we identify in this report.
The Legislature should amend state law to require BSCC to amend its regulations to ensure that county sheriff departments have mental health professionals perform incarcerated individuals’ mental health evaluations at intake and have staff conduct safety checks that are sufficiently detailed to determine that incarcerated individuals are alive.
The Legislature should amend state law to require the Sheriff’s Department’s Critical Incident Review Board to review natural deaths and develop a process to make public the facts discovered and recommendations made in response to all in‑custody deaths.
CLERB
To ensure that it completes investigations of all deaths that occur in the Sheriff’s Department’s custody within the one‑year time limit, CLERB should revise its rules and regulations by May 2022 to prioritize these investigations above all other investigations.
CLERB should revise its rules and regulations by May 2022 to include investigating natural deaths as part of its responsibilities.
Agency Comments
Although the Sheriff’s Department generally agreed with our recommendations, it questioned our audit approach and disagreed with our findings and conclusions. BSCC disagreed with our findings and recommendations but indicated that it would discuss whether amendments to its regulations are warranted. The Department of Justice and CLERB agreed with our recommendations.
Introduction
Background
The Sheriff’s Department’s Detention Facilities
- The department operates a system of seven detention facilities throughout San Diego County.
- Three of the detention facilities both process (book) individuals entering the jail system and house them.
- The other four facilities house individuals who are transferred after being booked.
- During our audit period from 2006 through 2020, the seven facilities collectively housed an average of about 5,200 individuals daily (average daily population) and booked an average of about 85,000 individuals annually.
Source: Sheriff’s Department documents and BSCC data.
The mission of the San Diego County Sheriff’s Department (Sheriff’s Department) is to provide high‑quality public safety services necessary to make San Diego the safest urban county in the nation. As the text box describes, the Sheriff’s Department operates a system of seven detention facilities. It also operates patrol stations, a crime laboratory, and an array of support operations. The Sheriff’s Department’s fiscal year 2020–21 adopted budget includes more than 2,000 employees who work in its detention facilities, including correctional staff (sworn staff), medical and mental health care staff (health staff), and administrative staff. In this report, we refer to all of these staff members collectively as detention staff.
San Diego County residents elect a sheriff to a four‑year term to serve as the chief executive of the Sheriff’s Department. The current elected sheriff has been in office since 2009. Under the elected sheriff’s guidance, the department must follow standards for jail conditions and treatment of incarcerated individuals set in regulation by the Board of State and Community Corrections (BSCC). The board also establishes local corrections training requirements and performs inspections of local detention facilities, to which the Sheriff’s Department is subject.
Deaths can happen in detention facilities for various reasons. The California Department of Justice asks counties to classify in‑custody deaths into seven main categories: natural death, homicide by law enforcement, homicide by other inmate, suicide, accidental death, pending investigation, or cannot be determined/other. Regardless of the category, different entities in San Diego County have responsibilities to prevent, respond to, and investigate deaths of incarcerated individuals, as we discuss below.
The Sheriff’s Department’s Role in Preventing and Responding to the Deaths of Incarcerated Individuals
Examples of Housing Types in the Sheriff’s Department’s Facilities
- Safety Cell/Enhanced Observation Housing: Temporary housing units constructed to maximize safety by removing physical features that could be used to inflict harm. These units are recommended for individuals who are actively self‑harming, assaultive, or at risk of suicide. Staff closely monitor individuals at random intervals.
- Medical Observation Beds: Beds located close to a nursing station for individuals whose condition necessitates hourly monitoring by health staff.
- Segregation Housing: Housing areas where individuals are placed in cells isolated from the general population and receive services and activities apart from others. Staff may place individuals in this housing for their own safety, staff safety, facility security, or pending a disciplinary action hearing.
- Mainline Housing: Housing areas for individuals who are classified as general population and therefore do not need to be isolated from others for security reasons or for medical or mental health reasons.
Source: Sheriff’s Department policies and procedures.
As Figure 1 shows, the incarceration process starts when a law enforcement officer arrests an individual in San Diego County and brings him or her to a jail for processing, which is also known as booking. One of the most important steps in the intake process that follows is the individual’s health screening. This screening is the Sheriff’s Department’s first opportunity to identify an individual’s medical and mental health needs. After this health screening, the next major step is classification, which determines an individual’s housing assignment. As the text box shows, the Sheriff’s Department has various types of housing in its facilities. An individual’s housing assignment is critical to safety and care because it indicates to detention staff whether that individual has special needs or characteristics that warrant precaution.
To determine an initial housing assignment, sworn staff interview the individual; review the person’s current booking information, complete criminal history, and past incidents in custody; and consider any information or instructions provided by health staff members regarding restrictions related to medical or mental health needs. The department may subsequently change an individual’s housing assignment if circumstances require reclassification.
Figure 1
The Sheriff’s Department’s Booking Process

Source: Sheriff’s Department policies and procedures.
Figure 1 description:
Figure 1 is a flowchart that shows the steps in the Sheriff’s Department’s booking process. In the first step, after an individual is arrested, the arresting officer transports him or her to one of the Sheriff’s Department’s three booking facilities. Next in the process, a registered nurse performs a preliminary medical and mental health screening to determine whether the individual is medically fit for bookings and to identify whether there are any known illnesses and medications. If the individual is experiencing a medical or mental health emergency that cannot be managed by the Sheriff’s Department, he or she may be sent to the hospital. Individuals in need of further evaluation or more urgent medical care will receive a secondary nurse assessment within a few hours of their first screening. Third in the process, based on the intake assessment, a nurse can write a mental health referral or schedule a medical follow-up with a doctor as needed, at a later date. Lastly, the individual proceeds to classification, which determines his or her housing assignment.
When individuals are in custody, the Sheriff’s Department is responsible for providing basic health care services and for performing safety checks at least every hour to provide for their health and welfare. Incarcerated individuals may request medical or mental health attention, or dental care, as needs arise. Providing care on an ongoing basis and performing adequate safety checks are vital to ensuring the safety of incarcerated individuals.
When an individual dies in the custody of the Sheriff’s Department, its homicide unit (homicide unit) investigates the death and assists the San Diego County Medical Examiner’s Office (Medical Examiner’s Office) by attending the autopsy and answering any questions surrounding the circumstances of the death. The Medical Examiner’s Office, an agency independent of the Sheriff’s Department, investigates all deaths of persons in custody. The Medical Examiner’s Office’s main function is to determine the manner of death—such as accidental—and the cause of the death—such as by drug overdose.
The Sheriff’s Department also performs other internal reviews of in‑custody deaths. For instance, within 30 days following a death, it must review the circumstances surrounding the incident and pertinent medical and mental health services and reports (30‑day medical review). It must also complete a critical incident review for all deaths except natural deaths. Most of these reviews could result in the Sheriff’s Department taking corrective action, such as changing policies or initiating employee discipline. We discuss the Sheriff’s Department’s internal reviews in detail later in this report.
The Citizens’ Law Enforcement Review Board’s Responsibilities Related to the Deaths of Incarcerated Individuals
CLERB’s Responsibilities
Investigating complaints against peace officers that involve the following allegations:
- Use of excessive force, discrimination, or sexual harassment towards members of the public.
- The improper discharge of a firearm.
- Illegal search or seizure.
- False arrest.
- False reporting.
- Criminal conduct or misconduct.
Reviewing, investigating, and reporting on the following incidents, regardless of whether a citizen files a complaint:
- The death of any individual arising out of or in connection with actions of peace officers.
- Incidents involving the discharge of a firearm.
- Use of force by peace officers resulting in great bodily injury.
- Use of force by peace officers at protests or other events protected by the First Amendment.
Source: CLERB rules and regulations.
The Citizens’ Law Enforcement Review Board (CLERB) is a key county entity that provides external oversight when an incarcerated individual dies in San Diego County. San Diego County voters amended the county charter in 1990 to require the County Board of Supervisors (county board) to establish CLERB to investigate complaints against officers employed by the Sheriff’s Department and Probation Department. CLERB’s mission is to increase the accountability of and public confidence in peace officers employed by the San Diego County’s Sheriff’s Department and the Probation Department. As the text box describes, CLERB is responsible for achieving its mission by conducting independent, thorough, timely, and impartial reviews of complaints of misconduct, among other things. This audit focuses only on CLERB’s investigations of deaths in the Sheriff’s Department’s jails. The San Diego County Charter establishes CLERB’s power to subpoena, administer oaths, and require the attendance of witnesses and the production of books and papers pertinent to its investigations.
CLERB currently consists of 11 board members nominated by San Diego County’s chief administrative officer and appointed by the county board for three‑year terms. Serving without compensation, CLERB members must be qualified electors of San Diego County, possess reputations for integrity and responsibility, and demonstrate an active interest in public affairs and service. County rules prohibit its employees or individuals employed as peace officers from serving. CLERB makes advisory findings on complaints and recommendations for policy and procedure changes to the sheriff, chief probation officer, and the county board. CLERB has also established rules and regulations to further facilitate its operations, which the county board has approved.
CLERB’s staff support the CLERB members by conducting complaint investigations, preparing written reports with findings and recommended policy changes, and transmitting the final reports to the Sheriff’s Department, Probation Department, and the county board. CLERB’s staff currently includes five special investigators, one supervising special investigator, an administrative secretary, and an executive officer. CLERB members appoint its executive officer, to whom they have delegated most of their authority over the other staff. CLERB’s executive officer must possess a bachelor’s degree and five years of management‑level experience. CLERB’s special investigators must have five years of experience performing investigations for a law enforcement agency, district attorney’s office, or other governmental agency or organization.
The Attorney General’s and County Board’s Oversight of the Sheriff’s Department
The county board is the governing body of San Diego County and is composed of an elected supervisor from each of the county’s five districts. State law gives the county board the authority to supervise the official conduct of all county officers, as well as officers of all districts and other subdivisions of the county, including CLERB. However, the county board’s oversight of the county sheriff has limitations, as Figure 2 shows. The California Constitution and state law provide that the county sheriff is an elected county official with certain independent functions and duties with which the county board cannot interfere. Nonetheless, state law establishes the county board’s budgetary authority over the Sheriff’s Department, and it also exercises some oversight—albeit minimal—through its establishment and oversight of CLERB.
Figure 2
The County and State Have Oversight of the Deaths of Incarcerated Individuals

Source: California Constitution, San Diego County charter, state law, CLERB’s rules and regulations, and Sheriff’s Department policies.
Figure 2 description:
Figure 2 shows the county and state entities that have oversight of the deaths of incarcerated individuals and descriptions of those responsibilities. The county board of supervisors is at the top of the graphic and the text next to it states that state law gives the county board the authority to supervise the conduct of all county officers, including CLERB members. However, the California Constitution and state law give the sheriff independent functions and duties with which the county board cannot interfere. There is a solid line from the county board of supervisors leading down to the Citizens’ Law Enforcement Review Board. CLERB is an eleven-member citizens’ board established by voter-approved proposition in 1990 (members appointed by county board). CLERB special investigators—who must have a least give years of investigative experience—review in-custody deaths and complaints of misconduct by officers of the Sheriff’s Department. Further, CLERB makes advisory findings and recommendations related to death cases—however, the Sheriff’s Department ultimately decides whether to take action. The board submits investigative reports to the county board and the Sheriff’s Department. A dotted line connects the county board of supervisors to the San Diego County Sheriff’s Department. The dotted line signifies that state law provides the county board with authority to approve the Sheriff’s Department’s budget, but it otherwise has limited authority over the Sheriff’s Department. The text related to the San Diego Sheriff’s Department describes that it performs various internal reviews after an incarcerated individual’s death. The Sheriff’s Department’s homicide unit investigates all types of deaths. Its Critical Incident review board reviews suicides, homicides, and accidental deaths, but not natural deaths. Further, its medical staff performs an assessment of care provided before each death. At the bottom of the graphic, with an arrow pointing to the San Diego Sheriff’s Department, text describes that the State also has oversight through the attorney general. The California Constitution designates the State’s attorney general as the chief law officer of the State. The attorney general may bring civil action to eliminate the pattern or practice of conduct by law enforcement officers that deprives any person of rights protected by law or the constitution. Further, sheriff’s departments must report in-custody deaths to the attorney general within 10 days.
Although the county board has limited oversight of the sheriff, the state constitution designates the State’s attorney general as the chief law officer of the State. Specific statutes describe the attorney general’s authority. For example, state law requires the Sheriff’s Department to report to the attorney general all facts concerning the death of an individual while in its custody within 10 days of that death. To ensure uniform and adequate enforcement of the laws of the State, the attorney general may also call into conference all of the sheriffs, district attorneys, and chiefs of police in the State for the purpose of discussing the duties of their respective offices. Further, the attorney general may bring a civil action to eliminate the pattern or practice of conduct by law enforcement officers that deprives any person of rights protected by law or the constitution. Finally, when necessary for the public interest, the attorney general is authorized to direct sheriff activities related to the investigation or detection of crime within a county.
Chapter 1
The San Diego County Sheriff’s Department Did Not Take Sufficient Steps to Prevent the High Number of Deaths in Its Jails
Chapter Summary
From 2006 through 2020, a total of 185 people died in San Diego County’s jails—one of the highest totals among counties in the State. The high rate of deaths in San Diego County’s jails compared to other counties raises concerns about underlying systemic issues with the Sheriff’s Department’s policies and practices. In fact, our review identified deficiencies with the way the Sheriff’s Department provides care for and protects incarcerated individuals that likely contributed to deaths in its jails. These deficiencies related to its provision of medical and mental health care, as well as its performance of checks to ensure the safety and health of individuals in its custody. When we evaluated the policies of three comparable counties, we found that some have adopted procedures that could address weaknesses we identified at the San Diego Sheriff’s Department. That said, the problems we identified with the Sheriff’s Department’s policies are in part the result of certain statewide corrections standards that are not robust or specific enough, leaving the establishment of effective practices to the discretion of the individual counties. Given that the annual number of incarcerated individuals’ deaths in county jails across the State increased from 130 in 2006 to 156 in 2020, improving the statewide standards is essential to ensuring the health and safety of incarcerated individuals in all counties.
In the Past 15 Years, More Individuals Died While in the San Diego Sheriff’s Department’s Custody Than in the Custody of Nearly Any Comparable County in the State
State data on deaths in custody at county jails show that San Diego County reported the second‑highest number of in‑custody deaths over the past 15 years. State law requires a law enforcement agency or an agency in charge of a correctional facility, including county sheriff’s departments, to report any case in which a person dies in its custody to the Office of the Attorney General within 10 days after the death. We present an interactive dashboard for viewing statewide data and additional detail regarding deaths in county detention facilities at https://www.auditor.ca.gov/reports/2021‑109/supplemental.html. It followed only Los Angeles County, which is significantly larger. Further, there continues to be a substantial number of deaths in San Diego County’s jails, as Figure 3 shows. Many of the individuals who died were in the Sheriff’s Department’s custody for only a few days to a few months before their deaths. Some of these individuals were awaiting trial, or scheduled to be released or transferred to state hospitals.
Figure 3
There Continues to Be a Substantial Number of Deaths in San Diego County’s Jails

Source: California Department of Justice in‑custody death data, BSCC data, and Sheriff’s Department information.
* We use the Sheriff’s Department’s information on in‑custody deaths in 2021 because it was not included in the California Department of Justice data, which is as of May 2021. We use ADP information from the Sheriff’s Department for 2021 because BSCC did not have complete ADP data for 2021.
Figure 3 description:
Figure 3 is a bar chart showing that there continues to be a substantial number of deaths in San Diego County’s jails. Each bar in the chart shows the number of deaths each year in the Sheriff’s Department’s jails from 2006 through 2021. The number of deaths ranged from eight in 2012 to as many as 18 deaths in 2021. Figure 3 also shows average daily population (ADP) for each year from 2006 through 2020 and ranged from about 3,900 in 2021 to 5,700 in 2017.
Average Annual ADP and Bookings
From 2006 Through 2020
| ADP | BOOKINGS | |
|---|---|---|
| Alameda Sheriff’s Office | 3,325 | 51,842 |
| Orange Sheriff’s Department | 5,877 | 59,263 |
| Riverside Sheriff’s Department | 3,668 | 54,025 |
| San Diego Sheriff’s Department | 5,162 | 85,631 |
Source: BSCC data and San Diego Sheriff’s Department bookings data.
In comparison to similar counties, more individuals died in the San Diego Sheriff’s Department’s custody in the past 15 years as Figure 4 shows. We identified the Alameda County Sheriff’s Office (Alameda Sheriff’s Office), Orange County Sheriff’s Department (Orange Sheriff’s Department), and Riverside County Sheriff’s Department (Riverside Sheriff’s Department) as comparable considering their size, geographical location, and other factors. The text box shows the average daily population (ADP) and bookings from 2006 through 2020 for each of these four counties.The ADP represents the number of incarcerated individuals housed in a jail system for any given day over a period of time and is used to determine whether a jail is operating at or near capacity. Bookings represent the total number of individuals who were processed through the county jail system. From 2006 through 2020, 185 incarcerated individuals died in the San Diego Sheriff’s Department’s jails, in comparison to 99 in the jails of the Alameda Sheriff’s Office, 111 in Orange Sheriff’s Department’s jails, and 104 in Riverside Sheriff’s Department’s jails. More recently, from 2016 through 2020, 72 people died while in the care of the San Diego Sheriff’s Department, whereas 25 people died in the care of the Alameda Sheriff’s Office, 46 in Orange Sheriff’s Department, and 37 in Riverside Sheriff’s Department. Even when considering each of these counties’ jail systems’ ADP and number of bookings, the rate of deaths reported by the San Diego Sheriff’s Department still exceeded that of the comparable counties. In fact, we reviewed data from the 15 largest counties in the State and found that the rate of deaths in San Diego County was among the highest.Appendix A provides the number and rate of deaths in the 15 largest counties in relation to their ADPs and bookings. Although any death is a tragedy, the high rate of deaths at San Diego County compared to other counties is particularly concerning.
Figure 4
Over the Past 15 Years, More Individuals Died in San Diego County’s Jails Than in Those of Comparable Counties

Source: California Department of Justice in‑custody death data and BSCC data.
We present interactive dashboards for viewing statewide data and additional detail regarding deaths in county detention facilities at https://www.auditor.ca.gov/reports/2021‑109/supplemental.html.
Figure 4 description:
The bar chart that shows that San Diego County Sheriff’s Department had 185 deaths in its jails compared to 99 deaths in Alameda County Sheriff’s Office’s jails, 111 deaths in Orange County Sheriff’s Department’s jails, 104 deaths in Riverside County Sheriff’s Department’s jails. Taking into consideration the rate of deaths based on the number of bookings and the ADP at each county jail system, San Diego still has the highest rate of deaths, both in the past 15 years and in the most recent five years. We also present interactive dashboards for viewing statewide data and additional detail regarding deaths in county detention facilities at https://www.auditor.ca.gov/2021-109/supplemental1.html
When we reviewed the manner of death, the San Diego Sheriff’s Department had a notably higher number of suicides and natural deaths than the comparable counties, as Table 1 shows.We present an interactive dashboard for viewing data on the age, race, and gender of the individuals who have died in each county detention facilities system at https://www.auditor.ca.gov/reports/2021‑109/supplemental.html.. Alarmingly, a total of 52 individuals in the San Diego Sheriff’s Department’s jails died by suicide over the past 15 years, which is more than twice the number in each of the comparable counties. Additionally, more individuals died of natural and accidental causes in the custody of the San Diego Sheriff’s Department than in the custody of each of the comparable counties, raising concerns about its ability to provide adequate safety and medical care to those it incarcerates. Natural deaths can include deaths from pre‑existing medical conditions and deaths resulting from inadequate care. After adjusting the comparisons based on each county’s ADP, the San Diego Sheriff’s Department still has historically had the highest rate of natural deaths and suicides.
Table 1
More Individuals in San Diego County’s Jails Died by Suicide or Natural Causes Than Individuals in the Custody of Comparable Counties
| MANNER OF DEATH | SAN DIEGO | ALAMEDA | ORANGE | RIVERSIDE |
|---|---|---|---|---|
| Total Deaths by County Sheriff’s Department From 2006 Through 2020 | ||||
| Accidental | 31 | 19 | 13 | 21 |
| Homicide (by law enforcement) | 4 | 0 | 1 | 2 |
| Homicide (by other inmate) | 8 | 4 | 4 | 6 |
| Natural | 88 | 52 | 77 | 51 |
| Suicide | 52 | 22 | 14 | 23 |
| Other | 2 | 2 | 2 | 1 |
| Totals | 185 | 99 | 111 | 104 |
Source: California Department of Justice in‑custody death data.
We present interactive dashboards for viewing statewide data and additional detail regarding deaths in county detention facilities at https://www.auditor.ca.gov/reports/2021‑109/supplemental.html.
Note: In San Diego County, accidental deaths mainly included drug overdoses. The two deaths shown as other include one pending investigation and one undetermined manner of death.
Based on data the Sheriff’s Department provided, in the most recent three years—2018 through 2020—the percentage of deaths of Black individuals in the Sheriff’s Department’s custody was disproportionately higher than their overall composition of the jail population. White individuals died at proportionally higher rates in 2007, 2009 through 2014, 2016, 2017, and 2020. In 2006, 2008, and 2015, the percentage of deaths among Hispanic individuals exceeded their population percentage. Although racial bias was not the focus of this report, our review of the Sheriff’s Department’s policies and procedures identified widespread deficiencies in its policies and practices for ensuring the health and safety of the individuals of all races and ages in its care.
Example of a Death That State Law
Does Not Require to Be Reported
July 1–An individual attempted suicide in a county jail but initially survived. The individual was transported to the hospital.
July 10–The sheriff’s department compassionately released the individual from custody.
July 15–The individual later died in the hospital as a result of the injuries from the attempted suicide.
Source: Records from sheriff’s departments.
We also found that sheriff’s departments did not report some deaths that occurred after incidents in jails because the individuals were released before their deaths. For example, we found instances in which the coroner or medical examiner’s offices described individuals dying in hospitals after incidents in the county jails, such as attempted suicide or medical emergencies. However, the respective counties did not report these deaths to the attorney general because the state law requiring reporting of in‑custody deaths requires sheriff’s departments to report only those individuals who died while in custody at the time of death and not individuals who died after having been released.For example, state law allows sheriff’s departments to compassionately release individuals from custody who would not reasonably pose a threat to public safety, and the incarcerated individual upon diagnosis by the examining physician, is deemed to have a life expectancy of six months or less. The text box provides an example in which sheriff’s departments would not need to report a death to the attorney general. Consequently, sheriff’s departments may be underreporting to the attorney general and to the public the number of deaths occurring from incidents in the jails.
The Sheriff’s Department’s Failure to Consistently Provide Adequate Care Likely Contributed to Its In‑Custody Deaths
We selected 30 individuals who died in the Sheriff’s Department’s jails from 2006 through 2020, weighted toward deaths that occurred in the last four years. Our selection included natural deaths, accidental deaths, suicides, and homicides.To comply with audit standards, we did not select cases involved in active litigation, including cases related to COVID‑19, in order to avoid interfering with ongoing legal proceedings. Although the Sheriff’s Department had reported one death in 2020 and one death in 2021 that were related to COVID‑19, it indicated that the manner of death has not yet been determined for 11 other cases in 2021, as of January 2022. Our review of the associated case files identified numerous problems with the Sheriff’s Department’s care of these individuals, starting with the inadequate health screenings it performed upon their initial arrivals through its insufficient responses to their medical emergencies, as Figure 5 shows. The deficiencies we identified in these areas for all types of deaths—including deaths classified as natural—suggest that the problems with the Sheriff’s Department’s care for incarcerated individuals are systemic.
Figure 5
Significant Deficiencies in the Sheriff’s Department’s Policies and Procedures Likely Contributed to the Deaths of Individuals in Its Custody

Source: The Sheriff’s Department’s jail records, surveillance videos, medical records, medical examiner reports, and homicide investigation documents related to a selection of 30 deaths of incarcerated individuals.
Figure 5 description:
An infographic that shows four significant areas of deficiencies in the San Diego’s policies and procedures that likely contributed to the deaths of individuals in its custody. The first area of deficiencies relates to insufficient health evaluations at intake. Specifically, health staff did not always properly identify incarcerated individuals’ medical and mental health needs at intake. Consequently, some of these individuals did not receive proper care, likely contributing to their deaths. The second area of deficiencies relates to inconsistent follow-up care. Specifically, detentions staff did not consistently follow up after individuals received or requested medical or mental health services, even though they often had serious needs that, when unmet, may have contributed to their deaths. The third area of deficiencies relates to inadequate safety checks. Specifically, sworn staff did not always adequately check on incarcerated individuals. Some individuals were found after their deaths, negating the opportunity for life-saving measures. The fourth and last area of deficiencies relates to unnecessary delays in performing lifesaving measures. Specifically, sworn staff’s and medical personnel’s slow response time to administer aid during medical emergencies may have contributed to unnecessary delays in lifesaving measures.
The assistant sheriff of detentions at the Sheriff’s Department asserted that the department is aware that its policies are not followed all of the time and recognizes that employees make mistakes, but it holds employees accountable when violations are discovered and makes every effort to provide additional training to prevent a recurrence. However, as the cases in our review show, failing to follow policies even in limited instances can result in the loss of life.
When we evaluated the policies at the Alameda Sheriff’s Office, Orange Sheriff’s Department, and Riverside Sheriff’s Department, we identified instances in which these entities have procedures that are more robust than those of the San Diego Sheriff’s Department. If the San Diego Sheriff’s Department followed these procedures, it could better ensure the health and safety of the individuals in its custody.
The Sheriff’s Department Did Not Ensure That It Identified Individuals’ Medical and Mental Health Needs at Intake
Because the Sheriff’s Department did not always properly identify the medical and mental health needs of individuals in our review at intake, some of them did not receive the care they required. Studies on health care at correctional facilities indicate that identifying individuals’ health needs at intake is critical to ensuring their safety in custody. For example, one of the keys to identifying potential suicidal behavior is through inquiry during the intake screening.
In at least eight of the 30 cases we reviewed, individuals had serious medical or mental health needs that health staff did not identify or communicate to detention staff at intake. Five of these individuals died within four days of their arrest. For example, in one case, an intake nurse determined that an individual needed to have a secondary nurse evaluation because the individual exhibited possible symptoms of drug withdrawal. However, there is no evidence in the case records that the intake nurse communicated this conclusion to other staff. The case records and video surveillance indicate that the individual died 24 hours after completing booking from complications resulting from a drug overdose without having seen another health professional.
In some of the cases we reviewed, the Sheriff’s Department did not promptly and properly identify individuals’ mental health needs because mental health professionals generally do not participate in its intake health screenings. Registered nurses perform the medical and mental health screenings at intake—asking both mental health and medical questions. These nurses are trained medically but do not necessarily specialize in mental health, which means that they may miss key signs of mental health needs. According to policy, if the registered nurse identifies an individual as having mental health needs at intake, the nurse refers the individual for further evaluation by a qualified mental health professional. However, even if the nurse identifies a need for a further mental health assessment, the Sheriff’s Department’s policy may not require the individual to receive that assessment sooner than 30 days after intake, depending on the severity of an individual’s symptoms. We noted one county had adopted more robust intake screening practices. Unlike the San Diego Sheriff’s Department, the Riverside Sheriff’s Department policy requires that a mental health clinician evaluate every individual before being housed, which could help to more effectively identify mental health needs early.
The San Diego Sheriff’s Department is currently advertising to hire additional mental health staff, and its director of mental health indicated that the Sheriff’s Department is aiming to have a qualified mental health professional, such as a mental health clinician or a psychologist, complete the mental health evaluations at intake. The county board approved additional funding in June 2021 for the Sheriff’s Department to hire a substantial number of additional nurses and mental health professionals.
In‑Custody Death: Case Example 1
An intake nurse did not identify an individual’s mental health needs and did not have access to the individual’s mental health history. Once incarcerated, that individual killed their cellmate.
After the cellmate’s death, the Sheriff’s Department discovered the perpetrator’s history of mental illness. Had staff known about this history, they likely would have placed the perpetrator in a different cell, where they could better meet the individual’s mental health needs and better ensure others’ safety.
Source: Records from the Sheriff’s Department.
In addition, the Sheriff’s Department’s intake nurses sometimes have not obtained complete medical and mental health history information on individuals. Although they may ask the individuals to sign a release of information that provides the department access to their medical and mental health records, individuals can refuse to sign. Historically, Sheriff’s Department nurses have not had immediate access to county health records, which could be key to identifying health needs at intake. For example, the text box describes a case involving two cellmates that resulted in one’s death. In this instance, a different outcome might have resulted had staff identified the perpetrator’s mental health history at intake.
The Sheriff’s Department entered into an agreement in September 2021 with the county Health and Human Services Agency to share behavioral health and medical information. The assistant sheriff of detentions stated that the Sheriff’s Department is in the process of getting access to this information. However, the Sheriff’s Department does not currently plan to require its intake nurses to look up each individual in the system. We believe this should be a standard step in the intake process to better ensure that the Sheriff’s Department has a more comprehensive health history for each individual who comes into its care. In fact, the Riverside Sheriff’s Department’s policy requires mental health staff to review Riverside County’s electronic health record system to determine whether an incarcerated individual has a history of receiving behavioral health care in Riverside County.
The Sheriff’s Department Did Not Consistently Follow Up With Individuals Who Needed Medical and Mental Health Services
Our case review found that Sheriff’s Department staff did not always follow up after individuals previously received or requested medical or mental health services, even though these individuals often had serious needs that, when unmet, may have contributed to their deaths. Best practices stress that timely treatment and follow‑up are important components of any health care system. Although the reasons that the Sheriff’s Department did not consistently follow up—such as poor policies and communication—varied by case, they represent deficiencies in its medical and mental health care system that it needs to address.
In some of the cases we reviewed, individuals reported to health staff that they were experiencing persistent symptoms, yet they did not receive timely evaluations from a physician. For example, in two cases involving natural deaths, individuals reported symptoms multiple times over the course of one to three weeks. Although these individuals were treated for a number of other medical and mental health issues, medical records show that they did not receive prompt attention from a physician for the symptoms that related to their deaths. Nurses originally assessed and treated these individuals for these symptoms. However, these individuals’ medical conditions worsened, and medical records show that they did not receive a physician’s evaluation before dying. Guidelines from the National Commission on Correctional Health Care (National Commission)—an organization that establishes standards for health services in correctional facilities—state that generally if an incarcerated individual reports to the nurse for evaluation more than twice for the same complaint and has not seen a physician, the individual should be scheduled to do so. However, this did not happen in these two cases. The Sheriff’s Department’s handling of these cases raises concerns over its follow‑up process for individuals experiencing persistent symptoms.
In other cases, potential deficiencies in the Sheriff’s Department’s policies related to mental and behavioral health treatment resulted in individuals not receiving services or needed follow‑up. For example, in one case, an incarcerated individual who had previously threatened suicide was released from a safety cell placement and enhanced observation housing. Although placement in a safety cell indicates that individuals are a danger to themselves or others, the Sheriff Department’s policy at that time did not specify time frames for ongoing follow‑up after such placement. In this case, mental health staff followed up only once with the individual after release from enhanced observation housing, and they assessed that the individual was low‑risk. Two weeks after the individual’s discharge from enhanced observation housing and about 12 days after the individual’s lone follow‑up encounter with a mental health clinician, the individual died by suicide.
Subsequently, the Sheriff’s Department revised its policy in 2019 for follow‑up care after release from a safety cell, but studies suggest that its revised policy may still be inadequate. Its revised policy delineates the follow‑up process for individuals after discharge from a safety cell or enhanced observation housing at a variety of intervals depending on certain conditions—every 24 hours, every three to seven days, and every seven to 14 days. Individuals may continue to receive follow‑up care at one of these intervals if certain conditions are met, including if it is their first time in detention, if they have recently attempted suicide, or if they have been charged with certain types of crimes. Although these follow‑ups can decrease in frequency, all of these individuals must have a follow‑up at least every 90 days. However, all individuals who have been placed into a safety cell or enhanced observation housing have demonstrated that they have significant mental health needs. While this policy is an improvement over its past policy, the Sheriff’s Department should reconsider the minimum ongoing follow‑up required. Reports and studies related to mental health indicate that more frequent psychological follow‑up, such as check‑ins performed weekly rather than every 90 days, leads to faster recovery and is more effective.
In‑Custody Death: Case Example 2
Day 1: At an intake screening, a nurse determined that an individual was mentally stable but initiated a referral for mental health services.
Day 2: The individual urgently requested mental health services. Staff denied the request, stating that the individual would be seen as soon as their referral was processed.
Day 4: The individual died by suicide without having seen a mental health professional.
Source: Records from the Sheriff’s Department.
Moreover, although the Sheriff’s Department’s policy indicates that a nurse should conduct a face‑to‑face appraisal with an incarcerated individual within 24 hours of a mental health care request to determine the urgency of that request, it has not always had this policy. As the case example in the text box describes, in one of the cases we reviewed the department’s weak policy likely contributed to the individual’s death by suicide, and the department revised this policy several months later. However, the revised policy still only requires a 24‑hour face‑to‑face appraisal for mental health requests, not medical health care requests. Therefore, inmates with urgent medical needs may not get prompt care. Best practices indicate that a face‑to‑face appraisal should apply to all nonemergency health care requests.
When we evaluated the policies of other counties, we identified a number of improvements the Sheriff’s Department should make to its policies and protocols related to following up on individuals’ medical and mental health care needs. For instance, the Orange Sheriff’s Department has a policy for assigning a behavioral health acuity level rating (acuity level rating) to each person who sees a mental health clinician during intake or whose mental health status alters during their stay in custody, necessitating a mental health assessment. This acuity level rating, which rates the severity of mental health needs, helps to inform housing location, the provision of mental health services, and discharge planning for when people leave custody. Such a system could help to identify mental health needs, track those needs, and communicate this information to appropriate staff to ensure that these needs are met, likely reducing the risk of death to the individual or others.
In addition, all three comparable counties have stronger policies for instances when incarcerated individuals refuse medical or mental health care. For some of the cases we reviewed, these refusals were frequent, despite the individual’s need for consistent care. The San Diego Sheriff’s Department and the three comparable counties have policies that require detention staff to witness and document an individual’s refusal to accept medical treatment or care. However, the Alameda Sheriff’s Office, Orange Sheriff’s Department, and Riverside Sheriff’s Department also require a health staff member to witness and sign the refusal. In contrast, San Diego allows a single sworn staff member to be the only signer if health staff are unavailable to serve as the second witness to the verbal refusal of care. Consequently, we identified several instances in which sworn staff were the only witnesses when incarcerated individuals refused to sign the refusals. Because follow‑up care is important, it is critical that the desire to refuse care be shared with health staff who are in a better position to ask appropriate questions, explain the adverse consequences to health that may occur as a result of the refusal, and assess whether an individual has critical health needs that should be addressed.
The chief medical officer of the Sheriff’s Department asserted that many of the issues we identified through our review are case‑specific and should not be used to draw generalizations about the department’s provision of health care. He also stated that the Sheriff’s Department has made a significant number of improvements to its health care system in recent years, such as adding an electronic medical record system and increasing physician and nursing support. He explained that the Sheriff’s Department is in the process of obtaining accreditation from the National Commission. To attain accreditation, the Sheriff’s Department must meet certain standards related to health care services and support, governance and administration, personnel and training, and other areas.
When the National Commission reviewed the Sheriff’s Department’s jails in 2017, it found that they did not meet many of its standards, particularly those related to mental health. The chief medical officer indicated that the Sheriff’s Department plans to contract with an outside health care organization to consolidate current services and expand its capabilities for the provision of comprehensive health care services, which may help it meet the requirements for accreditation. He further stated that the Sheriff’s Department is participating in a university research study that could lead to some facilities receiving accreditation sooner. Nonetheless, the department may be a couple of years away from obtaining full accreditation for all of its facilities.
Although seeking accreditation from the National Commission may address some of the problems we identify in this report, the Sheriff’s Department should not wait to implement key changes that would improve the safety of incarcerated individuals. We are concerned that this trend will continue if the Sheriff’s Department fails to quickly implement significant changes. In fact, the Sheriff’s Department indicated that the number of in‑custody deaths increased to 18 in 2021—the highest in 15 years.
The Sheriff’s Department Performed Insufficient Safety Checks
Performing safety checks is the Sheriff’s Department’s most consistent means of monitoring for medical distress and crime occurring in its jails. According to state law, local detention facilities must conduct safety checks at least hourly through direct visual observation of all incarcerated individuals. They must also have a written plan to document routine safety checks. Nonetheless, in our review of 30 in‑custody deaths, we found that sworn staff did not always perform safety checks adequately. As a result, they did not realize several individuals had died until hours afterward.
In fact, in several of the cases in our review for which the Sheriff’s Department has video files of safety checks, we found instances when sworn staff performed checks inadequately for the purpose of ensuring the safety of the individuals involved. Department policy requires that staff who are conducting safety checks look for any obvious signs of medical distress, trauma, or criminal activity. Although some video files were unavailable or incomplete for the 30 cases we reviewed, we reviewed the safety check logs and available video surveillance footage of sworn staff conducting checks.
In‑Custody Death: Case Example 3
2 a.m. Deputy quickly walked past each cell and glanced twice into the individual’s cell but moved on after the second glance.
3 a.m. Deputy stopped briefly at the individual’s cell, glancing through the window for a split second.
4 a.m. Deputy walked quickly past the individual’s cell without breaking stride, glancing through the window for less than a second.
5 a.m. Deputies found the individual unresponsive in their cell during a safety check, with signs of having died several hours earlier.
Source: Records from the Sheriff’s Department.
Based on our review of video surveillance footage, we observed multiple instances of sworn staff who spent no more than one second glancing into an individual’s cell, sometimes without breaking stride as they walked through the housing module, as we describe in the text box. Staff later discovered individuals unresponsive in their cells, some with signs of having died several hours earlier, as detention staff described some of these individuals as stiff and cold to the touch.
In another example, the Sheriff’s Department’s records indicate that a deputy did not perform a required safety check in a housing area, in part because of poor communication between this deputy and the station deputy. One hour after the deputy should have performed this check, sworn staff found an individual in this housing area unresponsive after attempting suicide. A physician pronounced this individual deceased at the scene after staff and paramedics were unsuccessful at saving the individual’s life.
Sworn staff conducted safety checks inadequately in part because of weaknesses in the Sheriff’s Department’s policy. Its safety check policy does not require sworn staff to determine whether individuals are alive and well by taking steps such as by observing the rise and fall of their chest. We recognize that acquiring proof of life in some situations is difficult and that waking up incarcerated individuals every hour could be detrimental to their well‑being. However, as described in the case example above, a safety check that does not involve any meaningful observation of an individual is ineffective and inadequate.
The Sheriff’s Department’s assistant sheriff of detentions indicated that the department’s policy is sufficient but that individual sworn staff members do not always follow it. The department’s safety check policy requires supervisors to review logs to ensure safety checks were logged and conducted at varying intervals within the required time periods, but it does not stipulate that this review should include examining video surveillance to confirm checks were conducted in a timely and appropriate manner. The assistant sheriff of detentions indicated that the department has an informal process for assessing the quality of safety checks, which can include watching video footage. However, the Sheriff’s Department has not documented this assessment process in its policy, and establishing an informal practice does not ensure that each facility’s management team will consistently verify the quality of safety checks.
The State and Orange Sheriff’s Department have more robust policies or additional detail in their policies that may be more effective in ensuring that incarcerated individuals are alive and well. For example, the California Department of Corrections and Rehabilitation (CDCR) requires staff who perform hourly checks to count a living, breathing person whom they see in person. Further, the Orange Sheriff’s Department requires staff who conduct safety checks to be close enough to each individual to ascertain the individual’s presence and apparent physical condition. According to Orange Sheriff’s Department’s assistant sheriff of detentions, a safety check must be performed from a sufficiently close vantage point to determine the person’s presence in their assigned location and whether the individual’s visible physical condition indicates the need for medical treatment or signs of being in medical distress. The detail described in these requirements could provide clearer expectations to San Diego Sheriff’s Department’s sworn staff for what constitutes an adequate safety check, especially during the night.
In addition, the Riverside Sheriff’s Department has a formal policy that requires regular video review of safety checks. For example, supervisors from each shift must randomly review two safety checks conducted during the prior shift. Establishing a similar process could help the San Diego Sheriff’s Department to identify sworn staff who do not consistently conform to policy when conducting their checks so that it can designate them for further action, such as additional training or disciplinary measures. Until it strengthens its safety check policy and formalizes a process for ensuring that sworn staff adhere to this policy, the San Diego Sheriff’s Department risks further instances of delayed responses to medical emergencies or other crises.
The Sheriff’s Department Did Not Always Provide Prompt Lifesaving Measures to Unresponsive Individuals
In slightly less than a third of the 30 cases we reviewed, issues with the response time of sworn staff or medical staff may have resulted in unnecessary delays in performing lifesaving measures. The early moments in a medical emergency are critical. A 2020 study found that one of the top five predictors of survival in a cardiac arrest occurring away from a hospital was someone performing cardiopulmonary resuscitation (CPR) immediately. Study from the Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. In addition, a 2021 study found that for each five‑minute delay in calling emergency medical services, the odds of surviving a cardiac arrest decreased by 41 percent. Study from the American Journal of Emergency Medicine. Nonetheless, in some of the cases we reviewed, sworn staff failed to begin CPR immediately or before the arrival of medical staff, or were slow to respond to the scene of the medical emergency.
In contrast to the Sheriff’s Department, CDCR requires its custodial staff to provide immediate life support to incarcerated individuals until medical staff arrive. It revised its policy in response to a 2005 California district court order requiring it to do so. The Sheriff’s Department’s chief medical officer acknowledged that sworn staff are trained to be first responders and agreed that they should begin CPR while waiting for health staff to arrive.
In‑Custody Death: Case Example 4
6:51 a.m. After the individual informed deputy about experiencing shortness of breath, deputy escorted the individual to a different area instead of medical clinic and then left area.
6:52 a.m. Individual collapsed in that area.
6:54 a.m. Deputies entered area to check on the individual.
7:00 a.m. Medical staff arrived. They began lifesaving measures within a few minutes.
7:10 a.m. Emergency medical personnel arrived.
7:33 a.m. Paramedics transported the individual to the hospital, where a doctor pronounced the individual deceased.
Source: Records from the Sheriff’s Department.
In addition, in some of the cases we reviewed, we noted a delay in the response time of sworn and medical staff when an individual was in medical distress. Sheriff’s Department policy requires that all detention staff are responsible for recognizing, reporting, and responding to an incarcerated individual’s emergency medical needs. The policy specifically requires that if an individual’s condition is believed to be life‑threatening, sworn staff must immediately alert on‑duty health staff, provide basic life support and first aid care, and place a 911 request for a paramedic emergency response. In one case we reviewed, the homicide unit’s investigation reported that an incarcerated individual indicated to a deputy that they were experiencing shortness of breath. The individual had recently been seen by health staff several times for these symptoms. According to the investigation, the deputy was somewhat familiar with the individual’s medical conditions but indicated he was not aware of certain treatment the individual previously received related to shortness of breath. Nevertheless, the deputy indicated that he believed that the individual was experiencing anxiety and escorted the individual to a different area instead of the medical unit. Shortly afterward, the individual collapsed and sworn staff did not respond for a couple more minutes, as the case example in the text box describes. A health staff member finally arrived several minutes later and began lifesaving measures within a few minutes. The individual was pronounced deceased shortly after arrival to the hospital.
In another example, our review of video surveillance footage—in combination with the homicide unit’s investigative report containing statements from involved staff and inmate witnesses—found that the first deputy did not arrive at the scene of the incarcerated individual in medical distress until about five minutes after another incarcerated individual went to alert staff. Sheriff’s Department medical staff did not arrive until five minutes after that. Paramedics—who are trained in advanced cardiac life support measures—did not arrive for another five minutes—a total of approximately 15 minutes after sworn staff were first alerted. According to the chief medical officer, some type of communication shortcoming may have delayed the arrival of medical staff, but the exact cause is unknown. However, the initial delay followed by the slow response time of medical staff may have been detrimental to the individual’s likelihood of survival. In the Sheriff’s Department’s interviews of witnesses, other incarcerated individuals commented on the slow response of department staff.
The last two examples we describe emphasize the need for the Sheriff’s Department to take action to ensure that it promptly responds to emergencies. Specifically, sworn staff need additional training for immediately starting CPR and how to properly alert medical staff.
The Sheriff’s Department’s Inadequate Policies Are in Part the Result of Weaknesses in Statewide Corrections Standards
As Figure 6 shows, weaknesses in statewide corrections standards likely contributed to the problems we identified with the Sheriff’s Department’s policies. The BSCC establishes in regulation the minimum standards for jail conditions and treatment of incarcerated individuals that local detention facilities must follow. Every local jail system in the State uses these standards as a basis to create policies for inmate safety and care, although counties may choose to make their policies more robust. However, some of these standards may not be adequate for ensuring incarcerated individuals’ health and safety. Further, BSCC’s inconsistent continuing education requirements may not be sufficient to ensure that sworn staff adequately care for incarcerated individuals. Given the increase in the annual number of in‑custody deaths across the State from 130 in 2006 to 156 in 2020, improving statewide standards related to health and safety and training requirements is essential to ensuring the health and safety of incarcerated individuals in all counties.
Figure 6
Poor Statewide Standards Contributed to Inconsistencies in the Sheriff’s Departments’ Policies

Source: State regulations and policies at Alameda, Orange, Riverside, and San Diego sheriff’s departments.
Figure 6 description:
A flow chart that shows that poor statewide standards contributes to inconsistencies in the Sheriff’s Department’s policies. At the top of the flow chart, it states that BSCC designs the minimum standards for treatment of incarcerated individuals to be a minimum that all counties can achieve, regardless of variation in resources at the local level. The next step in the flow chart states that the San Diego Sheriff’s Department and all other county sheriff’s departments develop their own policies for jails that comply with BSCC’s standards. The next step in the flow chart states that because BSCC’s standards are minimal, we found inconsistencies in the policies across the four counties we reviewed, with some policies going beyond the standard for than other, yet even these policies were still insufficient. For example, BSCC’s standard for safety checks requires an element that all four counties—Alameda, Orange, Riverside, and San Diego—include in their policies, but some counties include additional requirements not found in the other counties’ policies. Despite variation among counties, none of the policies nor the BSCC standard specify that staff are required to check for proof of life during safety checks.
Although the Sheriff’s Department’s policies generally align with BSCC’s standards related to health, safety, and personnel training, those standards are not specific enough in certain areas to ensure inmate safety. For example, BSCC’s standards do not explicitly require that a mental health professional should perform mental health screenings. As a result, the San Diego Sheriff’s Department’s, Alameda Sheriff’s Office’s, and Orange Sheriff’s Department’s policies allow medical nurses and health clinicians rather than mental health professionals to perform mental health screenings at intake. In these counties, the health staff generally will refer an incarcerated individual for a mental health evaluation if they observe general signs necessitating the referral or if the individual self‑reports mental health concerns. In contrast, the Riverside Sheriff’s Department’s policy requires a mental health professional to conduct the mental health screening in all instances, which is a best practice.
In another example, BSCC’s standards do not describe the actions that constitute an adequate safety check. Instead, the standards simply state that safety checks must be conducted at least hourly through direct visual observation of all inmates and that observation through a video camera alone is not sufficient. The four counties we reviewed based their policies on different interpretations of this standard, as Table 2 shows. The Alameda Sheriff’s Office and Riverside Sheriff’s Department require hourly direct visual observation of incarcerated individuals, but their policies do not expand much further on the standard. As we discuss previously, the San Diego Sheriff’s Department’s policy provides more detail, defining what staff should look for during the direct visual observation. The Orange Sheriff’s Department’s policy is more robust than the minimum standard: it directs sworn staff to be close enough to each individual to ascertain their presence and apparent physical condition. Moreover, CDCR requires its staff to count living, breathing individuals whom they see in person. This count is an hourly check that is the equivalent to what BSCC’s standards refer to as a safety check. Although BSCC is currently revising the safety check standard, its proposed revision still does not specify that a safety check must include verifying that an individual is alive, which is essential to ensuring the safety of incarcerated individuals across the State.
Table 2
A Lack of Specificity in Statewide Standards Has Resulted in Inconsistencies Among Counties’ Policies
| Entity With Policy | Safety Checks Policy Excerpt |
|---|---|
| BSCC | Safety checks shall be conducted at least hourly through direct visual observation of all incarcerated individuals. Observation through a video camera alone does not constitute a safety check. |
| Alameda Sheriff’s Office | Supervision of all incarcerated individuals shall include direct visual observation of each incarcerated individual by a deputy at random times each hour. |
| Orange Sheriff’s Department | A safety check is a direct visual observation of each incarcerated individual located in an area of responsibility every hour. Safety checks must be conducted from a location which provides a clear, direct view of each incarcerated individual. Staff shall be close enough to each incarcerated individual to ascertain his or her presence and apparent physical condition. |
| Riverside Sheriff’s Department | Security checks shall be completed to ensure there is direct visual supervision of all incarcerated individuals housed within a jail facility every hour. |
| San Diego Sheriff’s Department | Sworn staff will conduct safety checks of incarcerated individuals every hour through direct visual observation without the aid of audio and video equipment. Safety checks of incarcerated individuals consist of looking at the incarcerated individuals for any obvious signs of medical distress, trauma, or criminal activity. |
Source: State law and policies from the Alameda, Orange, Riverside, and San Diego sheriff’s departments.
Additionally, state law does not require that BSCC have medical or mental health professionals on its board, despite its responsibility for creating standards in these areas. The qualifications for almost all of the board member positions are related to law enforcement in a detention setting. State law requires BSCC to seek the advice of medical and mental health professionals when establishing minimum standards and when reviewing and making revisions every two years. However, because the standards have so much impact on the lives of incarcerated individuals, we believe that having medical and mental health representation on the board is critical. Similar boards in other states, such as the New York City Board of Corrections and the Texas Commission on Jail Standards, have medical experts serving as members.
In addition, BSCC’s required training hours for sworn staff working in local detention facilities do not align with their standards for similar positions. BSCC’s regulations require only 24 hours annually of continuing professional education training for adult correctional officers, supervisors, and managers, even though it requires 40 hours of continuing training for probation officers and juvenile correctional supervisors and managers. Requiring fewer hours for adult corrections personnel does not make sense when thousands of individuals are incarcerated in these facilities and the number of individuals who have died has increased over the past 15 years. Based on our review of how San Diego Sheriff’s Department's sworn staff responded to medical, mental health, and safety needs, we recommend increasing the number of training hours to align with similar professions to allow sheriff’s departments to better protect and keep incarcerated individuals safe. Further, BSCC does not require that any of the 24 hours of training cover topics pertaining to mental health, even though best practices suggest staff should receive at least four hours of mental health training annually. Without such a requirement, law enforcement staff may not be sufficiently prepared to provide care to and properly monitor individuals with mental health needs.
In response to our concerns that some of its standards are not robust enough to ensure the safety of incarcerated individuals in local detention facilities across the State, BSCC’s deputy director of Facilities Standards and Operations told us it is the responsibility of each individual county to establish policies that exceed the minimum standards, should they decide to do so. Further, she said that BSCC designs the standards to be a minimum that all counties can achieve, regardless of variation in resources at the local level. However, this approach enables counties that house large numbers of incarcerated individuals to provide lower levels of care. An alternative approach could be for BSCC to establish separate standards for counties with smaller incarcerated populations, and set higher standards for counties with larger incarcerated populations. For example, BSCC could create more stringent requirements for the larger counties in the State, such as those with ADPs of more than 1,000 individuals. This threshold would include the county jail systems housing more than 80 percent of the State’s jail population in local detention facilities. Further, some solutions—such as more robust safety checks—do not require significant resources. Improving statewide standards and training requirements is essential to ensuring the health and safety of incarcerated individuals in all counties.
Chapter 2
Neither the Sheriff’s Department Nor CLERB Has Taken Adequate Action in Response to the Deaths of Incarcerated Individuals
Chapter Summary
The Sheriff’s Department has not consistently taken meaningful action in response when in‑custody deaths have occurred. Specifically, its reviews of in‑custody deaths have been insufficient and have lacked transparency. As a result, the Sheriff’s Department risks conveying to the public that it is not taking these deaths seriously and making every effort possible to prevent similar deaths in the future. In addition, CLERB—a citizen‑governed board approved by San Diego County voters to restore public confidence in county law enforcement—has failed to provide effective, independent oversight of in‑custody deaths. In violation of its own rules and regulations, CLERB’s investigations of the deaths of individuals in the Sheriff’s Department’s custody have not been independent, thorough, or timely. Moreover, CLERB failed to investigate nearly a third of the deaths of incarcerated individuals in the past 15 years, meaning that dozens of deaths have not been subject to a key form of review outside of the Sheriff’s Department.
The Sheriff’s Department Has Not Consistently Implemented the Meaningful Changes Necessary to Respond to the Deaths of Individuals in Its Custody
The Sheriff’s Department has not responded to incarcerated individuals’ deaths in a manner that demonstrates its commitment to improving health and safety at its detention facilities. Every death of an individual in its custody should require a thorough review to determine whether changes to its processes are warranted. Nonetheless, the department’s reviews of deaths are insufficient and have not always led to meaningful corrective action. Further, although the Sheriff’s Department has implemented some key recommendations provided by external entities, it did not implement others that are critical to improving the safety of incarcerated individuals. San Diego County has paid millions of dollars in settlements related to deaths in the Sheriff’s Department’s jails that highlighted many of the same problems we have identified related to inadequate safety checks and medical and mental health care.
The Sheriff’s Department’s Processes for Investigating and Reviewing In‑Custody Deaths are Ineffective, Structurally Problematic, and Lacking in Transparency
The Sheriff’s Department has not performed adequate reviews or implemented sufficient changes in response to the deaths of incarcerated individuals. As we show in Figure 7, the department conducts up to four different reviews: a 30‑day medical review, a Critical Incident Review Board review, a homicide death investigation, and an internal affairs investigation. However, because all of these reviews are generated from within the Sheriff’s Department, they may be viewed by the public as lacking objectivity. Further, we identified deficiencies in certain reviews that call into question their ability to prompt meaningful change to prevent additional deaths.
Figure 7
The Sheriff’s Department’s Internal Reviews Have Not Led to Meaningful Action in Response to Individuals’ Deaths

Source: Sheriff’s Department’s policies and procedures and other documentation related to these reviews.
Figure 7 description:
A graphic showing a variety of the Sheriff’s Department’s internal reviews related to in-custody deaths and the deficiencies in those reviews. These four reviews have not consistently led to meaningful action in response to individuals’ deaths. The first review listed in the graphic is called the 30-day medical review. This review is performed by Sheriff’s medical staff within 30 days of the death as required by state law. For suicides, mental health staff also review the deaths. However, this 30-day medical review is not a formally documented report. Further, the review does not consistently document findings and recommendations and does not document follow-up to any recommendations. The second review listed in the graphic is called the Critical Incident Review Board review. This entity is within the Sheriff’s Department so it is not independent. During this review, staff present facts of the cases to Sheriff’s Department’s management and legal counsel. All reports are considered attorney-client privileged and are nondiscloseable. Further, the stated purpose of board is to assess liability. Additionally, the review board has not consistently taken meaningful action and does not review natural deaths. The third review listed in the graphic is the homicide investigation. These investigations are performed by Sheriff’s Department staff. In addition, these staff present facts of the case to the Critical Incident Review Board. The fourth and final review listed in the graphic is the internal affairs investigation. It becomes involved generally based on complaints of alleged misconduct. However, it has reviewed very few cases involving in-custody deaths.
One of the Sheriff’s Department’s reviews—the 30‑day medical review—involves reviewing the circumstances surrounding the incident and pertinent medical and mental health services and reports. According to state law, the Sheriff’s Department must review every in‑custody death within 30 days to determine the appropriateness of clinical care; to assess whether changes to policies, procedures, or practices are warranted; and to identify issues that require further study. To fulfill this requirement, Sheriff’s Department policy states that the medical services administrator, in consultation with the chief medical officer, is responsible for reviewing all in‑custody deaths within 30 days. In practice, the chief medical officer—who is a licensed physician—indicated that he currently conducts the reviews with input from other health staff regarding the individuals’ clinical histories. Although the chief medical officer is also required to review suicide deaths, the department’s policy has specified since late 2018 that the chief mental health officer will also present findings on suicides.
However, the Sheriff’s Department did not sufficiently document the results or recommendations from its 30‑day medical reviews. For 22 of the 30 cases we reviewed, the Sheriff’s Department was unable to provide us with documentation from these reviews that detailed any findings or conclusions about the clinical care given; identified whether any concerns required further study; or stated whether changes to policies, procedures, or practices were warranted. The documents we obtained for most of these 22 cases were either presentation slides or meeting agendas. Neither type of document included findings about the cases or recommended changes to policies, procedures, or practices. For some of the more recent cases in 2019 and 2020, the Sheriff’s Department provided us with the chief medical officer’s and medical staff members’ typed notes, which included conclusions about the medical care its staff had provided to the incarcerated individuals, as well as some recommendations. However, most of these reviews did not document whether the recommendations led to the department taking action, or whether the recommendations had been implemented.
We believe that if the Sheriff’s Department properly documented the 30‑day medical reviews, it could better identify and track instances when it did not provide sufficient medical and mental health follow‑up care before an individual’s death, such as those we discuss in Chapter 1. The chief medical officer agreed that the reviews, if properly documented, could be useful as an educational and quality assurance tool. However, he indicated that he would have reservations about formalizing these reports in a written format without some form of protection against using these documents as evidence in litigation. He stated that without such protection, staff members would be reluctant to point out any form of mistake or error, leading to lost learning opportunities. Regardless of the department’s position, we believe the reviews should be formalized for internal use to help the department better track its identification of deficiencies and recommendations for improvements to its clinical care. Other counties we reviewed have policies for documenting these 30‑day reviews.
In addition to the 30‑day medical review, in‑custody deaths—except natural deaths—are also subject to review by the Critical Incident Review Board, which is the Sheriff’s Department’s internal review committee. The board consists of three voting members—commanders from the Law Enforcement, Court Services, and Detention Services bureaus—and two nonvoting members—the chief legal advisor and a commander from the human resources bureau. The stated purpose of the board is to consult with the department’s legal counsel when an incident occurs that may give rise to litigation. Therefore, it appears that its primary focus is protecting the Sheriff’s Department against potential litigation rather than focusing on improving the health and welfare of incarcerated individuals.
Moreover, the board is an entity within the Sheriff’s Department, so it is not independent. The Sheriff’s Department’s investigators present to the board the facts and circumstances related to an in‑custody death. According to department policy, the board then carefully reviews the incident from multiple perspectives, including training, tactics, policies, and procedures. Its ultimate goal is identifying problem areas and recommending remedial actions—such as posting a training bulletin or changing a policy—so that potential liability can be avoided in the future. According to policy, if the board votes to determine that any policy violations exist, it will forward the case to Internal Affairs.
However, after the board meets to discuss in‑custody deaths, it has not always taken meaningful action to prevent deaths, even when it identifies problems with its policies and practices. Of the 18 cases we reviewed for which the department held a Critical Incident Review Board meeting, the board reported taking action related to 13. However, only six resulted in substantive actions, such as changes to policy and procedures or training, related to preventing inmate deaths. The remaining seven resulted predominantly in minor administrative actions or recommendations for training that would not have far‑reaching effects on the welfare of individuals in custody.
Moreover, even though the board discussed critical issues in some meetings, it ultimately concluded them without making recommendations for addressing these issues. For example, in six of the 18 cases, the board indicated that the events surrounding the deaths in question could merit changes to policy and procedures; however, it did not recommend any related actions. According to the assistant sheriff of detentions, the Sheriff’s Department may make immediate changes to policies following a death if it identifies a need, so additional recommendations from the board are sometimes unnecessary. However, the minutes of the Critical Incident Review Board meetings do not always discuss these types of policy changes. We question why the review board did not discuss the need for changes in some instances or discuss whether any changes made address the problems identified.
Further, the Critical Incident Review Board generally does not review natural deaths. Instead, it primarily reviews suicides, homicides, and accidental in‑custody deaths. According to the Sheriff’s Department’s chief legal advisor, the board does not review natural deaths in part because the risk of legal liability in those incidents is low. He further stated that because the Medical Examiner’s Office has made a determination that an individual’s death was from natural causes, it rules out other human factors. However, we found in our review of 30 case files that the Medical Examiner’s Office typically reviews events preceding individuals’ deaths and their medical records, but it does not make conclusions about the appropriateness of care provided by the Sheriff’s Department. We find the Sheriff’s Department’s decision not to hold critical incident reviews for natural deaths concerning given that these deaths accounted for nearly 50 percent of all deaths in the department’s facilities in the period of our review. Further, as we note in Chapter 1, we identified significant deficiencies in the Sheriff’s Department’s handling of care leading to all types of deaths, including natural deaths. By not requiring the Critical Incident Review Board to review these cases, the department is not doing everything it can to protect incarcerated individuals.
Finally, the Critical Incident Review Board is not transparent. It does not make its reports and investigations public. The board’s reports are classified as attorney‑client privileged, meaning that they are confidential and cannot be disclosed without the Sheriff’s Department’s consent. The purpose of attorney‑client privilege is to ensure that clients can fully disclose information to their lawyer without fear that it will be revealed to others, enabling them to receive competent legal advice. Although we do not disagree with having a confidential forum to discuss potential litigation matters, we are concerned that the Sheriff’s Department does not have a separate public process to demonstrate that it is addressing deficiencies in its policies, procedures, and practices after in‑custody deaths occur. By keeping its findings and recommendations confidential, the department risks conveying to the public that it is not taking these deaths seriously, investigating them thoroughly, or acting to prevent future incidents.
Although the Sheriff’s Department’s homicide unit is rarely involved in developing policy recommendations, it typically presents facts about in‑custody deaths to the Critical Incident Review Board. The homicide unit investigates deaths that occur in custody by, in part, inspecting the scene of the incident, interviewing any witnesses and detention staff, and reviewing video surveillance and reports written by sworn staff. Even though the information that the homicide unit presents to the Critical Incident Review Board is a key component of the Sheriff’s Department’s review of in‑custody deaths, the Critical Incident Review Board ultimately decides whether to take further action.
The Sheriff’s Department’s internal affairs unit may also investigate detention staff—including health staff—for alleged misconduct related to an in‑custody death. The internal affairs unit receives complaints that are initiated by a member of the community or by the Sheriff’s Department. The Critical Incident Review Board can also initiate an internal affairs investigation if it votes that a policy violation may have occurred.
However, the Sheriff’s Department has performed very few such investigations. Specifically, it reported to us that it conducted only four internal affairs investigations related to the 30 cases we reviewed, even though we identified a number of potential violations or concerns in some of the other 26 cases that could justify further investigation. Further, internal affairs indicated that it investigated staff conduct related to only 21 of the 185 in‑custody deaths that occurred from 2006 through 2020.
Thus, the Sheriff’s Department does not complete internal affairs investigations frequently enough for it to provide significant value. Although internal affairs indicates that its investigations are generally complaint‑driven, the small number of investigations related to death cases—coupled with the lack of meaningful changes arising from the 30‑day medical review and the Critical Incident Review Board meeting—calls into question the Sheriff’s Department’s commitment to protecting individuals in its custody.
The Sheriff’s Department Has Not Implemented Key Recommendations From External Entities Related to Incarcerated Individuals’ Welfare and Safety
The Sheriff’s Department has not implemented a number of key recommendations from external entities that are essential for ensuring the welfare and safety of incarcerated individuals, as Table 3 shows. We reviewed recommendations from 2006 through 2020 that the San Diego County Grand Jury, CLERB, Disability Rights California, and a suicide prevention consultant (consultant) made to the Sheriff’s Department. We discuss CLERB’s process for investigating deaths in the sections that follow. Many of these recommendations were in response either to a specific death or to the general health and safety conditions of the jails. When we looked at recommendations that pertained to the safety of incarcerated individuals, the Sheriff’s Department had implemented a number of them. For example, it modified a use‑of‑force policy to prevent compromising an incarcerated individual’s ability to breathe and revised its intake screening to include additional questions related to suicide prevention. However, some of the recommendations that the Sheriff’s Department failed to fully implement are connected to problems we identify in this report.
Table 3
The Sheriff’s Department Has Not Implemented Certain Key Recommendations From External Entities
| Entity Providing Recommendation | Example of Recommendation | Current Implementation Status |
|---|---|---|
| San Diego County Grand Jury–2014/2015 | The Sheriff’s Department deputy detention staff has an imbalance in experience levels and facility assignments, such as too many inexperienced staff at one facility. Develop and implement a staff rotation policy for all detention facilities. | Not implemented |
| Consultant reviewing suicide prevention practices–2018 | Given the strong association between in‑custody suicide and segregation housing and consistent with national correctional standards, it is strongly recommended that the Sheriff’s Department give strong consideration to increasing deputy rounds of such housing units from 60‑minute to 30‑minute intervals. | Not implemented |
| CLERB–2018 | Sheriff’s Department staff did not have pertinent information about an incarcerated individual’s previous suicide attempt and allowed that individual access to something that resulted in self‑harm and ultimately suicide. The Sheriff’s Department should revise its policy to use identifying wristbands to indicate a prior suicide attempt. | Not implemented |
| Disability Rights California–2018 | Revise policies to allow individuals in Enhanced Observation Housing to have access to social visits, increased out‑of‑cell time, and recreational activities, and to possess clothes and certain personal property, based on individualized clinical assessments of their condition and safety needs. | Not implemented |
Source: San Diego County Grand Jury reports from 2006 through 2019, a consultant’s report on suicide prevention practices, CLERB investigations and recommendations from 2006 through 2020, and a Disability Rights California report.
Specifically, the Sheriff’s Department did not implement recommendations related to safety checks, intake screenings, and suicide prevention efforts—the last of which is particularly concerning given the department’s high rate of suicides compared to other counties. For example, in response to a specific death, CLERB recommended in 2020 that the Sheriff’s Department require additional steps in safety checks of individuals residing in special mental health housing to ensure that they are alive and well, such as requiring nurses to accompany deputies on each round to ensure incarcerated individuals’ safety. However, the department stated it would not implement this recommendation because it believed that its current policies were adequate. Additionally, San Diego County contracted with a consultant in 2018 to assess suicide prevention practices within the Sheriff’s Department’s jail system. One of the consultant’s recommendations was for the Sheriff’s Department to consider increasing safety checks of individuals who are housed in isolated housing units from every 60 minutes to every 30 minutes, given the association between suicide and isolated housing placement. However, the department responded that making this change was not feasible because of the physical layout of its jail facilities, the number of inmates, and the required staffing.
The Sheriff’s Department’s justifications for choosing not to implement crucial recommendations have not always addressed the underlying issues involved and do not offer alternatives for addressing the concern. For example, following another death, CLERB recommended in 2018 that the Sheriff’s Department provide identifying wristbands to individuals with prior suicide attempts. In its response, the department indicated it would not implement this recommendation because doing so would violate individuals’ privacy and be contrary to best practices for suicide prevention. However, the Sheriff’s Department did not address or offer an alternative solution to the underlying problem, which is that sworn staff may not be familiar with the mental health histories of the individuals they oversee. As we discuss in Chapter 1, another county has addressed this problem by assigning individuals with mental health needs an acuity level rating that could help communicate this information to sworn staff.
Another key, recurring recommendation that the Sheriff’s Department has not implemented for nearly a decade relates to updating equipment for monitoring the safety of incarcerated individuals. In 2014 the San Diego County Grand Jury recommended that the Sheriff’s Department update the surveillance system for monitoring activity at its largest male detention facility, which is a maximum security jail. The San Diego County Grand Jury made a similar recommendation in 2017, but the department has yet to replace the system. Although the department’s policies and procedures related to facility maintenance generally align with state standards, we find it concerning that it has not yet replaced the surveillance system, even though its age is a major safety issue. In 2021 the Sheriff’s Department indicated that the replacement effort would likely not begin until the summer of 2022. According to the assistant sheriff of detentions, the department did not implement this recommendation sooner because of its prioritization of other projects, such as building a new detention facility. However, we believe that the Sheriff’s Department should prioritize implementing or resolving all recommendations intended to keep individuals in its custody safe.
Lastly, many of the lawsuits we reviewed that San Diego County settled have highlighted some of the same problems at the Sheriff’s Department that we have identified related to inadequate safety checks, mental health treatment, and medical care. From 2006 through 2020, there were 22 lawsuits filed related to the deaths of incarcerated individuals at the Sheriff’s Department’s detention facilities. San Diego County has settled 11 of these, for a total cost of $9.2 million.The other 11 lawsuits are either ongoing or have been appealed. Payments for these cases ranged from $10,000 to $3.5 million for an average of $838,000 per settlement. Table 4 compares San Diego County’s settlements to those in the other three counties we reviewed. By not promptly addressing the underlying issues on which both litigation and external recommendations have focused, the San Diego Sheriff’s Department continues to place the individuals in its custody at risk.
Table 4
Settlements Related to In‑Custody Deaths Varied Among the Comparable Counties
| Settlements Related to In‑Custody Deaths (2006–2020) |
Alameda | Orange | Riverside | San Diego |
|---|---|---|---|---|
| Number of settlements | 15 | 9 | 7 | 11 |
| Settlement amount (total) | $17,863,000 | $7,799,000 | $3,871,000 | $9,223,000 |
| Settlement amount (average) | $1,116,000 | $867,000 | $553,000 | $838,000 |
| Range of settlements | $10,000 to $5 million | $200,000 to $2.75 million | $46,000 to $975,000 | $10,000 to $3.5 million |
Source: Court documents from each of the four counties.
CLERB Has Failed to Provide Effective Oversight of the Deaths of Individuals in the Sheriff’s Department’s Custody
Despite its mission to increase public confidence in county law enforcement officers, CLERB has failed to provide effective, independent oversight of the deaths of individuals in the Sheriff’s Department’s custody. In violation of its own rules and regulations, CLERB’s investigations are not independent, timely, or thorough, as Figure 8 shows. Our review found that CLERB rarely independently interviews witnesses or visits the initial scenes of the deaths, has not consistently prioritized cases involving deaths, and has sometimes failed to thoroughly investigate or follow up on discrepancies it discovers in the course of its investigations of deaths. CLERB’s failure to conduct adequate investigations has resulted in a lack of independent scrutiny of dozens of deaths of incarcerated individuals, calling into question its effectiveness as a key oversight body for San Diego County law enforcement.
Figure 8
CLERB Has Failed to Provide Adequate Oversight of the Deaths of Individuals in the Sheriff’s Department’s Custody

Source: CLERB’s rules and regulations, county policies, and analysis of CLERB investigations.
Figure 8 description:
A graphic showing that CLERB has failed to provide adequate oversight over the Sheriff’s Department because its investigations, while ethical and fair/impartial, were not independent, timely, or thorough. CLERB’s rules and regulations require it to be independent, timely, thorough, ethical, and fair/impartial. However, the graphic shows that CLERB’s investigations were not independent, timely, or through. Its investigations are not independent because it primarily relies on evidence provided by the Sheriff’s Department, rather than independently interviewing witnesses or visiting the initial scene of the death. Its investigations are not timely because it has not always prioritized conducting investigations of death cases. Its investigations are not thorough because it does not always thoroughly investigate death cases or follow up on key discrepancies that arise during the investigation. We did not identify concerns with the investigations we reviewed being conducted in an unethical manner or being unfair or biased.
CLERB Does Not Conduct Independent Investigations
San Diego County voters established CLERB to provide independent oversight of the county’s law enforcement agencies. However, CLERB’s investigations of in‑custody deaths are not independent. In particular, it does not conduct interviews with Sheriff’s Department sworn staff or visit the initial scene of the death. Rather, it relies almost entirely upon documents that the Sheriff’s Department provides. The county charter—as well as its own rules and regulations—establishes CLERB’s power to issue subpoenas, administer oaths, and require the attendance of witnesses and the production of books and papers pertinent to its investigations. CLERB’s rules and regulations further state that its investigations may include interviewing witnesses and subject officers, examining the scene, and reviewing and preserving other physical evidence. However, in practice, CLERB’s investigations of in‑custody deaths reflect neither its authority nor its stated processes.
CLERB uses these questionnaires in lieu of performing in‑person interviews as the result of an agreement it reached with the Sheriff’s Department and the Deputy Sheriff’s Association of San Diego County (labor organization). However, this agreement has hindered CLERB’s independence and undermined voters’ approval of CLERB’s creation. As we show in Figure 9, the erosion of CLERB’s independence began in the 1990s. According to CLERB’s current executive officer, CLERB was concerned at that time that its investigations were one‑sided and lacked legitimacy without participation by Sheriff’s Department sworn staff. According to its annual reports and internal documents, CLERB attempted to interview Sheriff’s Department sworn staff in the course of its investigations to seek their perspective. Although both San Diego County’s Administrative Code and CLERB’s rules and regulations entitle CLERB to complete and prompt cooperation from the Sheriff’s Department, the sworn staff members refused to participate in interviews with CLERB investigators. In response, CLERB exercised its power to subpoena and administer oaths by calling sworn staff members to testify in public hearings. However, CLERB documents indicate that the sworn staff continued to refuse to answer any questions, invoking their Fifth Amendment right against self‑incrimination.
Figure 9
CLERB’s Ability to Conduct Independent Investigations Has Been Eroded Over Time

Source: Proposition voter materials, agreement documents, legal documentation, and CLERB’s investigations documentation.
Figure 9 description:
This timeline shows that CLERB’s ability to conduct independent investigations has been eroded over time. The timeline starts with 1990 and states that voters approved Proposition A to create a CLERB and give it power to subpoena and require attendance of witnesses and the production of books and papers pertinent to its investigations, as well as to administer oaths. The timeline next covers 1991 through 1995 and states that sworn staff involved in CLERB investigations refused to answer questions, citing their Fifth amendment rights, and CLERB defended itself against litigation related to its authority to perform investigations. The next stop in the timeline is 1998 and states that CLERB, the Sheriff’s Department, and the labor organization agreed to a process for CLERB investigators to question sworn staff through interviews or written questionnaires. In 2003 CLERB adopted a waiver form allowing sworn staff to opt out of participating in in-person interviews with its investigators. Lastly, in 2021 CLERB continues to not directly interview sworn staff involved in in-custody deaths, compromising the independence and thoroughness of its investigations.
Faced with the prospect of more costly litigation and continued legal challenges, CLERB discussed a framework with the Sheriff’s Department and the labor organization in 1998 that ultimately led to an agreed‑upon process for CLERB investigators to question Sheriff’s Department sworn staff through interviews or written questionnaires (1998 agreement). Further, in 2003, CLERB adopted a waiver form for sworn staff, allowing them to opt out of in‑person interviews with CLERB investigators altogether (2003 waiver form).
The 1998 agreement and 2003 waiver form constitute CLERB’s current process for involving Sheriff’s Department sworn staff in its investigations. Consequently, CLERB investigators do not conduct independent interviews of sworn staff but rather request responses from specific department employees through a written questionnaire. This approach has hindered CLERB’s ability to perform independent investigations.
CLERB’s executive officer acknowledged that having its investigators conduct independent interviews would be preferable but also asserted that they are generally able to obtain necessary information through the questionnaire process. However, we question this position. Although written responses may provide some pertinent information, they do not allow investigators to assess the credibility of a witness or to ask immediate follow‑up or clarifying questions. In fact, CLERB’s current process allows department staff up to 14 days to respond to the questionnaires. CLERB’s executive officer indicated that investigators generally submit another questionnaire with the same turnaround time if they have any subsequent inquiries or clarifying questions to the responses from the initial questionnaire. Such protocol is counterintuitive to the nature of an investigation, which requires interactive communication and prompt responses.
Moreover, although the Sheriff’s Department generally notifies CLERB of in‑custody deaths, it does not do so until after various department entities have processed the scene. As a result, CLERB investigators are not able to be present at the initial scene of the death. Instead, shortly after receiving notification of an in‑custody death, CLERB issues a subpoena to the Sheriff’s Department for the homicide unit’s investigation file. The Sheriff’s Department forwards it to CLERB once it has completed its criminal investigation, usually about two to eight months after the death occurs. As a result, CLERB’s investigators generally do not learn about potential witnesses or have the opportunity to visit the scene until months after the death of an incarcerated individual, severely limiting their ability to conduct an independent and thorough investigation. In fact, when we reviewed a selection of CLERB’s investigations, we found that its investigators either did not visit the scenes of the deaths at all or did not do so until more than a year after the death occurred.
Without the ability to independently interview witnesses or the opportunity to visit the initial scenes of the deaths, CLERB must conduct its investigation based primarily on information that the Sheriff’s Department’s internal investigators provide, such as photographs and videos. For the cases we reviewed, CLERB’s investigators' only other sources of evidence were statements from the decedents’ families, reports from the medical examiner, and—in only one case—a direct interview with an incarcerated individual who was a witness.
San Diego County voters established CLERB in response to perceived inadequacies in the Sheriff’s Department’s internal investigations, yet CLERB’s nearly exclusive reliance on evidence provided by the department precludes its investigators from reaching independent conclusions on in‑custody deaths and providing truly external oversight of county law enforcement. For CLERB to carry out this function, its processes must change and the Sheriff’s Department must fully cooperate.
CLERB’s members and its executive officer are currently pursuing several policy changes to increase its independence, including issuing a policy recommendation in October 2021 to the Sheriff’s Department requesting that it allow a CLERB staff member with extensive death investigation experience to be present at the initial scene of the death. However, CLERB’s recommendations to the Sheriff’s Department are advisory and require the Sheriff’s Department’s approval for implementation. CLERB’s members and executive officer are also working with the county board to expand CLERB’s authority to investigate complaints against non‑sworn staff, including medical personnel. However, such an expansion of CLERB’s authority requires approval by the county board. Furthermore, although these changes would increase the independence of CLERB’s investigations, they would not enable CLERB’s investigators to directly interview sworn staff, which we believe is critical.
CLERB Failed to Investigate 57 In‑Custody Deaths From 2006 to 2017
CLERB failed to investigate a significant number of deaths of individuals in Sheriff’s Department custody. For example, CLERB failed to investigate 13 deaths of incarcerated individuals from 2011 through 2016 because it misinterpreted a state‑mandated deadline for completing its investigations and did not properly prioritize its caseload. The Legislature established a one‑year statute of limitations for investigations of law enforcement misconduct when it amended the Public Safety Officers Procedural Bill of Rights Act (POBR) in 1997. As the Introduction explains, CLERB is responsible for investigating complaints, as well as deaths arising out of or in connection with actions of peace officers, which can include deaths in custody. As a result of the amendment to POBR, CLERB must complete its investigations within one year after it receives a complaint against a peace officer or notification of an in‑custody death.POBR requires the investigation to be completed within one year of discovery of the alleged misconduct, and the one‑year deadline may be suspended under certain circumstances, such as when the misconduct is the subject of a criminal investigation. Because the Sheriff’s Department performs a criminal investigation of every in‑custody death, CLERB’s one‑year time frame to complete its investigation does not start until after the Sheriff’s Department completes its investigation.
Nevertheless, CLERB did not realize until 2010 that the one‑year time frame applied to its investigations of complaints, at which time it started to dismiss cases for expiration of this time limit. In fact, from 2010 through 2016, CLERB reported that it had to dismiss nearly 100 complaints against county law enforcement members because it did not complete its investigations within the required time frame. Although CLERB did not report that any of these 100 complaints involved in‑custody deaths, its failure to conduct these investigations demonstrates that it has struggled to effectively perform its duties in a timely manner.
Further, CLERB’s records and San Diego County Grand Jury documents indicate that CLERB staff were not aware that the POBR statute of limitations also applied to its investigations of in‑custody deaths until 2017. Consequently, it did not always prioritize these cases, and it reported that its backlog of open investigations of deaths steadily increased from seven cases in 2010 to 46 cases by 2016. After CLERB learned in 2017 that the one‑year time limit also applied to investigations of deaths, it had to dismiss 22 of these cases because they had exceeded the time limit. Of these 22 deaths, 13 occurred while the individuals were in custody at Sheriff’s Department detention facilities.The remaining nine deaths occurred in San Diego County law enforcement areas and probation facilities. Because of CLERB’s failure to investigate these 13 deaths, it did not have the opportunity to identify problems with the Sheriff’s Department’s policies and procedures and to make policy recommendations that could have helped prevent future in‑custody deaths.
CLERB did not investigate an additional 40 in‑custody deaths classified as natural from 2006 through 2016 because it was not conducting investigations of this type during that time. According to CLERB’s current executive officer, it did not review deaths classified as natural during this period because its former executive officers generally interpreted its jurisdiction over in‑custody deaths to exclude these types of deaths. In fact, CLERB’s rules and regulations do not clearly specify whether CLERB should investigate natural deaths. However, the concerns we discuss with the Sheriff Department’s inadequate prevention of natural deaths underscore the importance of CLERB providing external oversight of these cases. Since 2017 CLERB has been consistently reviewing natural deaths. However, the lack of specificity in its rules and regulations could result in CLERB reverting to its past practice in the future.
In addition, CLERB did not investigate four other in‑custody deaths—two that were classified as accidental, one as homicide by law enforcement, and one as suicide—from 2009 through 2011. CLERB’s executive officer said that it did not investigate these deaths because the Sheriff’s Department failed to inform CLERB of their occurrence. Although the Sheriff’s Department indicated that it did not have information on notifications for this period, we find the lack of review of these cases concerning. In 2011 CLERB made a policy recommendation requesting that the Sheriff’s Department include it in all in‑custody death notifications. Although the Sheriff’s Department declined to modify its policies to include CLERB in its initial death notifications, which includes the county district attorney and Medical Examiner's Office, it did direct a specific unit to inform CLERB of all in‑custody deaths, usually within a few days of their occurrence. However, as we discuss above, when the Sheriff’s Department does not notify CLERB of deaths immediately, CLERB investigators do not have the opportunity to visit the initial scenes of the incidents shortly after the death occurred.
As we show in Figure 10, CLERB failed to investigate a total of 57 deaths of incarcerated individuals in Sheriff’s Department jails from 2006 through 2017—nearly a third of all its in‑custody deaths in the past 15 years. This is unacceptable given that CLERB is a key county entity outside of the Sheriff’s Department that reviews in‑custody deaths. Although CLERB recently added policies and procedures establishing its prioritization of death cases over all other cases, it did not do so until August 2021. Moreover, because policies can easily be changed when leadership changes, it is important that CLERB include requirements in its rules and regulations for how it prioritizes cases.
Figure 10
CLERB Did Not Investigate Nearly a Third of All In‑Custody Deaths in the Past 15 Years

Source: California Department of Justice in‑custody death data, CLERB list of investigations, and CLERB investigative reports.
Figure 10 description:
A graphic showing that over the past 15 years, CLERB did not investigate 57 of 185 deaths—or nearly a third of in-custody deaths—in San Diego County jails for three different reasons. The graphic uses an equation to distinguish between the deaths not reviewed for the given reasons. First, CLERB did not investigate 13 deaths because the statutory one-year time limit for completing the investigations expired. Next, CLERB did not investigate 40 deaths because it did not believe it needed to investigate natural deaths. Lastly, CLERB did not investigate four deaths because the Sheriff’s Department failed to inform CLERB of their occurrence. Adding together 13, 40, and 4 results in 57 deaths not reviewed.
Despite CLERB’s efforts since 2017 to ensure that it appropriately prioritizes and fully investigates in‑custody deaths, it has still struggled to complete its investigations in a timely manner. As we previously explained, CLERB investigators generally begin investigating an in‑custody death after the Sheriff’s Department’s homicide unit has completed its own investigation and forwarded the homicide investigation file to CLERB. Upon receipt of the homicide investigation file, CLERB must complete its investigation within one year to meet the POBR time limit. However, our review of the six in‑custody death investigations found that CLERB investigators did not begin their casework until an average of seven months after they received the homicide investigation file from the Sheriff’s Department. As we note earlier, the Sheriff’s Department usually does not provide the file to CLERB until two to eight months after the death of an incarcerated individual. Consequently, CLERB investigators did not complete their investigations of the cases we reviewed until an average of nearly a year and a half after the death occurred.
CLERB’s executive officer indicated that CLERB staff have not historically prioritized beginning investigations of deaths, but he has made recent efforts to ensure that staff start their investigations as soon as they receive a homicide file. Although CLERB’s policy does not provide instruction for how quickly the staff must start working on investigations of deaths, the executive officer told us that his goal is for these investigations to be complete within 90 days of CLERB receiving the homicide investigation file. To make relevant recommendations and hold individuals accountable for wrongdoing, CLERB must take steps to complete its investigations of in‑custody deaths in a timely manner.
CLERB Did Not Always Thoroughly Investigate In‑Custody Deaths
CLERB’s rules and regulations require its investigations to be thorough. However, in some of the cases we selected, CLERB’s investigators did not appear to consider all the circumstances leading up to the deaths, did not examine all the relevant Sheriff’s Department policies, and did not follow up on discrepancies they discovered in the course of their investigations. For example, in one case, an altercation between two cellmates resulted in the death of one of the individuals. However, the investigator did not appear to scrutinize or independently verify evidence, such as the victim’s mental health history, that might have affected their classification status. Without this information, the investigator could not sufficiently determine whether the Sheriff’s Department had violated policies or procedures by housing these individuals in the same cell. Consequently, the investigator found that there was no evidence to support an allegation of a procedural violation, misconduct, or negligence on the part of the Sheriff’s Department.
When failing to thoroughly examine all the evidence in a case, CLERB investigators may miss important opportunities to identify deficient policies and practices and to make recommendations to improve the safety of incarcerated individuals. CLERB’s executive officer explained that because CLERB investigators are often working against the POBR statute of limitations, they do not consistently follow up on discrepancies they discover in the course of their investigations. However, we find this explanation problematic given the critical nature of the investigations. Further, as we previously discuss, investigators often failed to begin their investigations until months after receiving the homicide files. By starting their investigations sooner, they could increase the time available to them.
Although CLERB developed policies and procedures in August 2021 that outline specific documents—such as medical records—investigators should obtain in the course of an in‑custody death investigation, we believe further action is necessary. Specifically, CLERB should develop a comprehensive training manual for its investigators that includes guidance for evaluating the circumstances leading up to the death, such as the decedent’s mental health history and the appropriateness of the decedent’s housing assignment. Such changes could help ensure that its investigations are complete and thorough.
Until Recently, the County Board Provided Insufficient Oversight of CLERB
The county board has a number of responsibilities related to CLERB. It appoints CLERB members and can remove individual members by a majority vote at any time. The county board also establishes CLERB’s duties and approves its rules and regulations. However, despite its critical role in overseeing CLERB, the county board rarely discussed in‑custody deaths or raised concerns about CLERB, based on its meeting minutes from 2006 through 2019, including after CLERB dismissed 22 death cases in 2017.
The county board has only recently begun to discuss in‑custody deaths. Its current chair stated that the board’s composition changed recently and that it now has an increased interest in addressing deaths in San Diego County jails. In 2020 the county board approved changes intended to strengthen CLERB’s oversight of the Sheriff’s Department and Probation Department, including increasing the number of investigative staff. It also approved a request for CLERB to revise its member nomination process to make it more transparent and better incorporate community input.
Although the current county board has recently been more engaged in monitoring in‑custody deaths, CLERB has not effectively communicated the pressing issues related to deaths in county jails to the county board. The county charter requires CLERB to prepare an annual report for the county board, the sheriff, and the county probation officer that summarizes its activities and recommendations, including the tracking and identification of trends with respect to complaints received and investigated. Even though CLERB has included in its annual reports year‑to‑year comparisons of the number of new death cases and complaints, its reports lack critical information that would enhance their usefulness. For example, the reports summarize information on the causes of death and certain categories of allegations of misconduct but do not include any significant discussion or analysis that might point to deficiencies in the Sheriff’s Department policies or practices. Further, they do not include any demographic information related to deaths that CLERB investigates.
Although CLERB’s reporting and recommendation practices generally align with requirements in its rules and regulations, it could make its annual reports and recommendations more useful. Other law enforcement oversight entities in the State include more robust information in their annual reports, such as comprehensive analyses and discussions of overall trends in discrimination, misconduct, and excessive force allegations, as well as demographic information. Additionally, as an advisory board, CLERB’s primary means of improving the safety of incarcerated individuals and providing oversight of in‑custody deaths is the recommendations for policy or procedural changes that it makes to the Sheriff’s Department based on the deficiencies it detects in the course of its investigations. However, CLERB generally makes recommendations based on individual cases rather than on trends it identifies through analysis of its investigations. Making recommendations based on trends could help resolve more systemic concerns at the Sheriff’s Department.
CLERB’s executive officer indicated that he would like to include more analyses of overall trends in the annual report but explained that he has prioritized other issues, such as resolving the case backlog and developing training materials for new investigators. As a key oversight entity for county law enforcement, CLERB must improve its reporting and analyses to better inform county leadership and the public. Even more importantly, it must make recommendations that address systemic issues to help prevent deaths of incarcerated individuals.
Conclusions and Recommendations
The San Diego Sheriff’s Department has a constitutional responsibility to provide adequate medical care to the individuals whom it incarcerates. Nonetheless, more people have died while in its custody over the past 15 years than in nearly any other county in the State—an average of about one death per month. Our audit found that deficiencies in the Sheriff’s Department’s policies and practices related to intake screenings, medical and mental health care, safety checks, and responses to emergencies likely contributed to these deaths. The high rate of deaths in San Diego County jails compared to other counties’ jails suggests that these systemic deficiencies have undermined the Sheriff’s Department’s ability to ensure the health and safety of the individuals in its custody. We are concerned about whether the Sheriff’s Department will make meaningful changes to address these systemic problems. Although external entities—such as CLERB and the San Diego County Grand Jury—have made recommendations in the past to address some of the deficiencies we describe, the Sheriff’s Department has not implemented a number of them.
No single entity has sufficient oversight authority over the Sheriff’s Department to require it to make meaningful changes. Absent explicit legislative direction, neither the county board nor the State’s attorney general is well positioned to compel the Sheriff’s Department to implement the recommendations we include in this report. Given the ongoing risk to incarcerated individuals’ safety, we believe that the Legislature should direct the Sheriff’s Department to implement the changes we detail below.
Recommendations
Legislature—All Sheriff’s Departments and the California Department of Justice
To ensure that all sheriff’s departments accurately report deaths that occur from incidents or conditions in county jails, the Legislature should amend state law to require sheriff’s departments to report to the attorney general individuals who are released from custody after being transported directly to a hospital or similar medical facility and subsequently die in the facility. It should also amend state law to require sheriff’s departments to provide the attorney general with all facts concerning the death, such as the cause and manner. The California Department of Justice should annually publish this information on its website.
Legislature—San Diego Sheriff’s Department
To ensure that the San Diego Sheriff’s Department identifies individuals’ medical and mental health needs at intake, the Legislature should require it to revise its policies to better align with best practices, as follows:
- Revise its intake screening policy to require mental health professionals to perform its mental health evaluations. These evaluations should include a mental health acuity level rating scale to better inform individuals’ housing assignments and service needs while in custody. The Sheriff’s Department should communicate the acuity level rating it assigns to individuals to all detention staff overseeing them.
- Create a policy requiring health staff to review and consider each individual’s medical and mental health history from the county health system during the intake screening process.
To ensure that the Sheriff’s Department provides the necessary medical and mental health care to individuals incarcerated in its facilities, the Legislature should require it to do the following:
- Revise its policy to require that nurses schedule an individual for an appointment with a doctor if that individual has reported to the nurse for evaluation more than twice for the same complaint.
- Revise its policy to require that a nurse perform and document a face‑to‑face appraisal with an individual within 24 hours of receipt of a request for medical services to determine the urgency of that request.
- Revise its policy to require more frequent psychological follow‑up after release from the inmate safety program, including at least monthly check‑ins.
- Revise its policy to require that a member of its health staff witness and sign the refusal form when an individual declines to accept necessary health care.
To ensure that sworn staff properly perform safety checks, the Legislature should require the Sheriff’s Department to do the following:
- Revise the safety check policy to include the requirement for staff to check that an individual is still alive without disrupting the individual’s sleep.
- Develop and implement a policy requiring that designated supervising sworn staff conduct audits of at least two randomly selected safety checks from each prior shift. These audits should include a review of the applicable safety check logs and video footage to determine whether the safety checks were performed adequately. In addition, the policy should require higher‑ranking sworn staff to conduct weekly and monthly audits of safety checks. The policy should also require each facility to maintain a record of the safety check audits that staff members perform.
To ensure that department staff promptly respond to unresponsive individuals, the Legislature should require the Sheriff’s Department to revise its policies to require that sworn staff members immediately start CPR without waiting for medical approval, as safety procedures allow. The Legislature should also require that the Sheriff’s Department provide sworn staff with additional training for starting CPR immediately and how to properly alert medical staff.
To ensure that the Sheriff’s Department properly assesses the reasons for each in‑custody death and makes prompt changes as necessary in response, the Legislature should require it to revise its policy to specify the following:
- Staff will provide a written report of each 30‑day medical review to its management.
- When warranted, the report should specify recommendations for changes to prevent further deaths.
- The 30‑day medical review should determine the appropriateness of clinical care; assess whether changes to policies, procedures, or practices are warranted; and identify issues that require further study.
To improve oversight of in‑custody deaths and encourage meaningful action to prevent future deaths, the Legislature should require the Sheriff’s Department to revise its policy to require that the Critical Incident Review Board review natural deaths.
To increase the transparency of the Sheriff’s Department’s reviews of in‑custody deaths, the Legislature should require the Sheriff’s Department to either make public the facts it discusses and recommendations it decides upon in the relevant Critical Incident Review Board meetings or to establish a separate public process for internally reviewing deaths and making necessary changes.
To ensure that the Sheriff’s Department provides complete and prompt assistance to CLERB’s investigations, the Legislature should require the Sheriff’s Department to do the following:
- Revise its policy to include CLERB in its immediate death notification process.
- Revise its policy to allow a CLERB investigator to be present at the initial death scene.
- Revise its policy to encourage its staff to cooperate with CLERB’s investigations, including participating in interviews with CLERB’s investigators.
The Legislature should implement the recommendations related to the Sheriff’s Department described above in a manner consistent with the form of governance applicable to San Diego County.
Legislature—BSCC
To ensure that standards of care for incarcerated individuals are adequate and consistent across the State, the Legislature should amend state law to require BSCC to amend certain regulations to address the following:
- County sheriff’s departments with jails that have an average daily population of more than 1,000 must have a mental health professional perform mental health evaluations at intake.
- Safety checks must include a procedure for checking to see that each individual is alive.
To ensure the involvement of experts in the areas of medical and mental health care in approving BSCC’s regulations and training standards related to the health and safety of incarcerated individuals, the Legislature should change the composition of BSCC to include a medical professional and a mental health professional.
To ensure that BSCC’s regulations, guidance, and training align with medical and mental health care best practices, the Legislature should require BSCC to evaluate and update all of its regulations and training as needed once its composition includes a medical professional and a mental health professional.
To ensure that all local correctional officers in the State receive sufficient continuing professional education, the Legislature should require BSCC to amend its regulations to require that local correctional officers working in local detention systems with an average daily population of more than 1,000, complete 40 hours of training annually and that at least four of those hours relate to mental and behavioral health.
CLERB
To ensure its investigations are independent, timely, and thorough, CLERB should do the following by May 2022:
- Discuss and modify its current agreement with the Sheriff’s Department and the labor organization to allow CLERB’s investigators to conduct independent interviews of Sheriff’s Department sworn staff.
- Develop a comprehensive training manual for its investigators that outlines standard procedures for investigations. The manual should include a specific section dedicated to investigations of in‑custody deaths, including guidance for evaluating the circumstances leading up to an in‑custody death, such as the decedent’s mental health history and the appropriateness of the decedent’s housing assignment.
- Create policies and procedures to require its investigators to finish casework on in‑custody death investigations within three months of receiving the homicide investigation file. These policies and procedures should also require investigators to attempt to independently verify any information they receive from the Sheriff’s Department, to thoroughly review deputy statements and reports from the homicide investigation file, and to request interviews with relevant detention staff and other witnesses in all instances in which they identify discrepancies or missing information.
To ensure that it fully investigates all in‑custody deaths, CLERB should revise its rules and regulations by May 2022 to include the following:
- Prioritization criteria for investigating in‑custody deaths above all other investigations.
- Clarification that its investigations of in‑custody deaths includes those classified as natural deaths.
To ensure that it provides effective oversight of the deaths of individuals in the Sheriff’s Department’s custody, CLERB should perform an analysis of overall trends related to these deaths, including demographic information, and determine whether the trends suggest deficiencies in the Sheriff’s Department’s policies and procedures. Based on these trends, it should also identify policy recommendations for improving the safety of the individuals in the Sheriff’s Department’s custody. To increase transparency, CLERB should include these trends and analyses in its annual reports starting with its 2021 report, which it should publish in 2022.
We conducted this performance audit in accordance with generally accepted government auditing standards and under the authority vested in the California State Auditor by Government Code sections 8543 et seq. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on the audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
Respectfully submitted,
MICHAEL S. TILDEN, CPA
Acting California State Auditor
February 3, 2022
Appendix A
In‑Custody Deaths in California’s 15 Largest Counties
The Joint Legislative Audit Committee (Audit Committee) directed us to compare the in‑custody death rate in San Diego County to the rates in other comparable California counties for the past 15 years—2006 through 2020. Table A.1 presents the rate of deaths per average daily population (ADP) in each of these county sheriff jail systems from 2006 through 2020. As we previously explain, the ADP represents the number of incarcerated individuals housed in a jail system on any given day over a period of time.
Table A.1
In‑Custody Deaths and ADPs From 2006 Through 2020
| County Sheriff’s Department | ADP 15‑Year Average (2006–2020) |
Total Deaths |
Average Deaths per Year |
Average Deaths per 1,000 ADP |
|---|---|---|---|---|
| San Diego | 5,162 | 185 | 12.33 | 2.39 |
| Fresno | 2,752 | 86 | 5.73 | 2.08 |
| Ventura | 1,537 | 47 | 3.13 | 2.04 |
| Kern | 2,266 | 69 | 4.60 | 2.03 |
| Alameda | 3,325 | 99 | 6.60 | 1.98 |
| Contra Costa | 1,446 | 43 | 2.87 | 1.98 |
| Riverside | 3,668 | 104 | 6.93 | 1.89 |
| San Francisco | 1,492 | 39 | 2.60 | 1.74 |
| San Joaquin | 1,367 | 34 | 2.27 | 1.66 |
| Los Angeles | 17,044 | 421 | 28.07 | 1.65 |
| San Bernardino | 5,490 | 124 | 8.27 | 1.51 |
| Santa Clara | 3,732 | 84 | 5.60 | 1.50 |
| Orange | 5,877 | 111 | 7.40 | 1.26 |
| Tulare | 1,510 | 26 | 1.73 | 1.15 |
| Sacramento | 4,008 | 62 | 4.13 | 1.03 |
Source: California Department of Justice in‑custody death data and BSCC data.
We present information on additional counties in our interactive dashboards at https://www.auditor.ca.gov/reports/2021‑109/supplemental.html.
Table A.2 presents the rate of deaths per the number of individuals booked in each county sheriff’s jail system from 2006 through 2020. The number of bookings is the total number of individuals who were processed through the jail system.
Table A.2
In‑Custody Deaths and Bookings From 2006 Through 2020
| County Sheriff’s Department | Total Booked |
Average Booked per Year |
Total Deaths |
Total Deaths per 100,000 Booked |
|---|---|---|---|---|
| Los Angeles | 1,970,654 | 131,377 | 421 | 21.36 |
| Fresno | 551,624 | 36,775 | 86 | 15.59 |
| San Diego | 1,284,462 | 85,631 | 185 | 14.40 |
| Kern | 520,074 | 34,672 | 69 | 13.27 |
| Riverside | 810,376 | 54,025 | 104 | 12.83 |
| Alameda | 777,627 | 51,842 | 99 | 12.73 |
| Orange | 888,951 | 59,263 | 111 | 12.49 |
| Santa Clara | 682,010 | 45,467 | 84 | 12.32 |
| San Bernardino | 1,027,195 | 68,480 | 124 | 12.07 |
| Contra Costa | 370,299 | 24,687 | 43 | 11.61 |
| Ventura | 424,978 | 28,332 | 47 | 11.06 |
| San Francisco | 353,521 | 23,568 | 39 | 11.03 |
| San Joaquin | 392,895 | 26,193 | 34 | 8.65 |
| Sacramento | 733,275 | 48,885 | 62 | 8.46 |
| Tulare | 333,941 | 22,263 | 26 | 7.79 |
Source: California Department of Justice in‑custody death data, BSCC data, and San Diego Sheriff’s Department bookings data.
Appendix B
Scope and Methodology
The Audit Committee directed the California State Auditor to conduct an audit of the San Diego Sheriff’s Department to determine the reasons for in‑custody deaths of incarcerated individuals and identify the steps taken by the Sheriff’s Department to address these deaths. The table below lists the objectives that the Audit Committee approved and the methods we used to address them.
Audit Objectives and the Methods Used to Address Them
| AUDIT OBJECTIVE | METHOD | |
|---|---|---|
| 1 | Review and evaluate the laws, rules, and regulations significant to the audit objectives. | Reviewed and evaluated the laws, rules, and regulations related to detention facilities and significant to the audit objectives. |
| 2 | Evaluate the Sheriff’s Department’s policies and procedures on personnel training, facility maintenance and safety, and the provision of health care to incarcerated individuals. To the extent possible, determine whether these policies and procedures align with minimum standards established through state law and any other applicable guidance. As part of this evaluation, also determine whether any of these policies delay or otherwise impair the ability of medical personnel to provide appropriate medical care to incarcerated individuals. |
|
| 3 | To the extent possible, for a selection of in‑custody deaths from the past 15 years—including suicides, murders, and in‑custody or in‑transit deaths—determine the following: a. The circumstances, such as the cause for each death. b. Whether correctional facility staff followed applicable policies and procedures related to in‑custody safety. c. Whether the Sheriff’s Department reviewed the circumstances of these deaths and took corrective action to improve in‑custody safety. |
|
| 4 | To the extent possible, evaluate available demographic information—including the race and age of the incarcerated individuals—and identify any relevant trends for all in‑custody deaths from the past 15 years. Compare the in‑custody death rate in San Diego County to the rates in other comparable California counties. |
|
| 5 | Review allegations from the past 15 years that led to wrongful death suits and determine the number of settlements, the average settlement amount, and, to the extent possible, how settlement awards compare to similar settlements from other comparable counties in California. |
|
| 6 | To the extent possible, determine which policies specified in settlement agreements or in grand jury recommendations have been implemented and which have not. As part of this determination, also identify whether the Sheriff’s Department has suspended, revoked, or amended any such policies in a manner inconsistent with past settlement agreements or grand jury recommendations. |
|
| 7 | Evaluate the extent to which CLERB has provided recommendations to the Sheriff’s Department regarding in‑custody safety and followed up to determine whether the Sheriff’s Department has implemented those recommendations. |
|
| 8 | Evaluate CLERB’s review of in‑custody death cases in 2017 and assess whether CLERB had sufficient staff and resources to perform its oversight role appropriately. |
|
| 9 | Review and assess any other issues that are significant to the audit. | None identified. |
Source: Audit workpapers.
Assessment of Data Reliability
The U.S. Government Accountability Office, whose standards we are statutorily obligated to follow, requires us to assess the sufficiency and appropriateness of computer‑processed information we use to support our findings, conclusions, and recommendations. In performing this audit, we relied on electronic data files that we obtained from the California Department of Justice related to in‑custody deaths in jails of the San Diego Sheriff’s Department, the Alameda Sheriff’s Office, the Orange Sheriff’s Department, and the Riverside Sheriff’s Department from 2006 through 2020. To evaluate the data, we reviewed existing information about the data, interviewed staff knowledgeable about the data, and performed testing of the data. Specifically, we compared data from the counties and the California Department of Justice to data we obtained from the Medical Examiner’s Office and coroner’s office in each respective county.
Although the state law requiring reporting of in‑custody deaths does not require sheriff’s departments to report deaths after an individual is released from jail, as we discuss here, we found that the data supporting the number of in‑custody deaths from the California Department of Justice related to the San Diego Sheriff’s Department and the Orange Sheriff’s Department to be sufficiently reliable for our audit purposes. We found some inaccuracies in the categorization of manner of death, but the inaccuracies do not change our conclusion, and therefore the data are sufficiently reliable for our audit purposes. We performed limited testing of the Alameda Sheriff’s Office’s and the Riverside Sheriff’s Department’s data and found them to be of undetermined reliability because of how the counties record and track the information. Although this determination may affect the precision of the numbers we present, there is sufficient evidence in total to support our findings, conclusions, and recommendations.
In addition, we obtained data from BSCC related to the ADPs and annual bookings of the San Diego Sheriff’s Department, the Alameda Sheriff’s Office, the Orange Sheriff’s Department, and the Riverside Sheriff’s Department. We used these data to identify and compare the number of in‑custody deaths at each department, taking into consideration the number of individuals incarcerated in its jail facilities. We interviewed staff knowledgeable about the data and performed general testing of the data. We found the data to be of undetermined reliability because the data are self‑reported from each county to BSCC. However, we found that the San Diego Sheriff’s Department overreported to BSCC the bookings data for 2006 through 2010. Therefore, we obtained additional data from the Sheriff’s Department to more accurately reflect bookings in our analyses. Although this determination may affect the precision of the numbers we present, there is sufficient evidence in total to support our findings, conclusions, and recommendations.
Lastly, we obtained statewide data from the California Department of Justice and BSCC related to in‑custody deaths and ADP for presentation on our interactive dashboards. We found the data to be of undetermined reliability because the data are self‑reported by each county. The dashboard is for informative purposes only; we do not present findings, conclusions, or recommendations on it.
Response to Audit
Board of State and Community Corrections
January 14, 2022
Honorable Michael S. Tilden
Acting California State Auditor
621 Capitol Mall, Suite 1200
Sacramento, California 95814
SUBJECT: RESPONSE – SAN DIEGO COUNTY SHERIFF’S DEPARTMENT AUDIT REPORT 2021-109
Dear Mr. Tilden,
The Board of State and Community Corrections is required to establish minimum standards for local detention facilities. (Pen. Code, § 6030.) Providing for safe and constitutional facilities is central to the Board’s regulations, which are continuously examined and revised on a biennial basis. The Audit of the San Diego County Sheriff’s Department (Report 2021-109) focuses on deaths in custody, which is a topic of utmost concern that merits serious attention. Having not been given an opportunity to review the findings in San Diego as part of this response, we are unable to comment on whether the deaths in custody in San Diego County were caused by the county adhering to BSCC regulations that were deficient or whether other operational or personnel issues may have contributed to the audit findings. The Board will undertake a review once the unredacted findings are available to determine to what extent the Board’s existing regulations merit revision. However, we disagree with the Auditor’s conclusions that the Board’s existing training standards are inadequate and that the BSCC’s regulations for the operation of adult local detention facilities that are proposed to be revised are insufficient for maintaining the safety of people who are incarcerated.
①Mental Health Screenings
The Auditor states the Board’s standards are insufficient to maintaining the safety incarcerated individuals, specifically citing that the regulations “do not explicitly require that mental health professionals perform mental health screenings.” We assume the Auditor is referring to “intake screenings,” where Section 1207 of Title 15 of the California Code of Regulations provides:
With the exception of inmates transferred directly within a custody system with documented receiving screening, a screening shall be completed on all inmates at the time of intake. This screening shall be completed in accordance with written procedures and shall include but not be limited to medical and mental health problems, developmental disabilities, tuberculosis and other communicable diseases. The screening shall be performed by licensed health personnel or trained facility staff, with documentation of staff training regarding site specific forms with appropriate disposition based on responses to questions and observations made at the time of screening. The training depends on the role staff are expected to play in the receiving screening process.
This regulation is aligned with National Commission on Correctional Health Care (NCCHC) J-E-02 which allows for “receiving screening to be conducted by health-trained correctional staff members when health staff are not on duty.” NCCHC standards are nationally recognized as best practice.
In addition, Sections 1206 and 1209 of Title 15 of the California Code of Regulations detail requirements of additional mental health screenings that may occur after the initial screening at intake. These requirements do require licensed medical and mental health care professionals to conduct mental health screening and require facilities to provide care for persons with mental health needs.
The Auditor appears to recognize that it may be impractical or impossible for all local detention facilities to have mental health professionals on staff 24/7 for intake, so the report recommends that facilities with average daily populations of 1,000 be required to have these requirements because counties with smaller incarcerated populations have “less risk.” While larger counties may be able to provide a higher level of service than other counties, establishing lesser standards for smaller counties is problematic and would create additional inequities within county criminal justice systems.
②Safety Checks
The Auditor argues that the current safety check regulation (and proposed revisions) are insufficient to protect the safety and welfare of inmates. The Auditor points to the fact that some counties’ policies are more detailed than the Board’s regulations. In addition, the Auditor notes the California Department of Corrections and Rehabilitation (CDCR) requires its staff to count “living, breathing” individuals. The fact that some counties may elect to explicitly detail what goes into a safety check in its policies does not mean the Board’s minimum standards do not provide for adequate safety. The Board’s regulations are designed to give counties flexibility to address their needs while adhering to constitutional standards. In addition, it is important to note that the requirements for counting individuals in the CDCR Department of Operations Manual (§§ 52020.5.5 and 52020.5) are not “safety checks.” They are merely instructions on staff to ensure a proper population count.
Section 1027.5 of Title 15 of the California Code of Regulations requires a written plan at each facility that includes documentation of safety checks. Title 15 section 1006, Definitions, provides detail for how safety checks must be conducted and defines both direct visual observation and safety checks:
“Direct visual observation” means direct personal view of the inmate in the context of his/her surroundings without the aid of audio/video equipment. Audio/video monitoring may supplement but not substitute for direct visual observation.
“Safety checks” means direct, visual observation performed at random intervals within timeframes prescribed in these regulations to provide for the health and welfare of inmates.
As part of the most recent regulation revisions adopted at the most recent BSCC board meeting, the Board revised section 1027.5 to require enhancements to safety checks, which, once approved by the Office of Administrative Law, will read, as follows:
§ 1027.5 Safety Checks.
The facility administrator shall develop and implement policy and procedures for conducting safety checks that include but are not limited to the following:Safety checks will determine the safety and well-being of individuals and shall be conducted at least hourly through direct visual observation of all people held and housed in the facility.
(a) There shall be no more than a 60- minute lapse between safety checks.
(b) Safety checks for people in sobering cells, safety cells, and restraints shall occur more frequently as outlined in the relevant regulations.
(c) Safety checks shall occur at random or varied intervals.
(d) There shall be a written plan that includes the documentation of all safety checks. Documentation shall include:
- the actual time at which each individual safety check occurred;
- the location where each individual safety check occurred, such as a cell, module, or dormitory number; and,
- Initials or employee identification number of staff who completed the safety check(s).
(e) A documented process by which safety checks are reviewed at regular defined intervals by a supervisor or facility manager, including methods of mitigating patterns of inconsistent documentation, or untimely completion of, safety checks.
In this revision, the regulation will explicitly require that safety checks "determine the safety and well-being of individuals." The BSCC revised regulation exceeds many other states' safety check regulations, and is aligned with best practices for safety checks.
In short, safety checks allow for potential interventions when people are in distress, but it is also important to balance the needs of people who are incarcerated from overly intrusive and unnecessary checks. Counties have been subject to litigation over allegations of failing to conduct adequate safety checks and also for unnecessarily interrupting sleep as part of rigorous safety check programs. The Board’s regulation and proposed revision strikes the appropriate balance in providing for the safety of people who are incarcerated and meeting county operational needs.
③Training Standards
The Auditor states that the BSCC’s training standards are insufficient for maintaining the safety of incarcerated individuals. The Auditor solely relies on the total increase in the number of deaths in county jails from 2006 to 2020 to conclude training is insufficient. Based on the information provided in the redacted report, the BSCC is unable to determine whether a lack of specific training caused any of the deaths examined in San Diego and to what extent additional training requirements would have been beneficial or prevented these situations. Instead, the report states that “weaknesses in statewide corrections standards likely contributed to the problems we identified with (redacted) policies” without any specific detail. Without a clear nexus between a deficiency in the training standards and a bad outcome such as a preventable death, it is incorrect to assume that higher standards will better ensure the health and safety of incarcerated individuals.
The Auditor states that the Board’s continuing education requirements across job classifications (adult correctional officer, juvenile correctional officer, and probation officer) are inconsistent and recommends that the adult correctional officers should receive 40 hours of annual training on par with probation officers. In addition, the Auditor recommends that agencies with average daily populations of 1,000 or more should require 4 hours of mental health training annually.
The characterization of the continuing education requirements as inconsistent is incorrect. BSCC sets standards for adult corrections officers, juvenile corrections officers, and probations officers and their managers and supervisors. Those jobs are not interchangeable nor are their training requirements. The “inconsistencies” noted in the report are deliberate decisions based on the differences in positions. Requiring the same number of hours across all classifications is arbitrary and not based on job-specific requirements. Furthermore, the number of required hours for the adult corrections officer is on trend nationally and exceeds the number of continuing education hours required by the California Commission on Peace Officer Standards and Training for other peace officer positions.
The report recommends that continuing education include a minimum of 40 hours training annually and at least four hours of mental health training for adult corrections officers for agencies with an ADP of 1,000. First, it should be noted that the BSCC standards already require 21 hours of Behavioral Health training for every officer upon hire. It includes training in suicide prevention, stigma and bias, trauma, emotional survival, interventions and resources, and recognizing signs and symptoms of mental illness and trauma.
Second, we question the premise that more hours of annual training, regardless of the topic or need, will always yield better results. Continuing education hours are deliberately left to the discretion of the agency so that they can identify the specific training needs of an employee, including performance management, and to support organizational priorities or training gaps. Training is not a static need and it should remain flexible to ensure critical gaps are addressed. Training is a critical tool that can improve employee performance and organizational success. However, it is only effective when used appropriately. Problems must be assessed to determine if training can be an effective part of the solution. Culture, ineffective policies, and employees deliberately acting outside of policy are some examples of when training is not an appropriate solution. The portions of the audit we were able to review do not provide an assessment that shows that what was at issue in San Diego was a training failure that will improve by mandating four hours of mental health training each year for all adult corrections officers.
Finally, as with the recommendation to have lesser screening standards for smaller counties, we also disagree with setting lesser training standards for correctional officers in smaller counties.
To be sure, the BSCC continually evaluates the need for entry-level training and annual training. We will take the recommendation under advisement when evaluating the next revision of our training standards to determine whether adding annual mental health training would be beneficial.
In closing, the BSCC appreciates the Auditor’s review of its standards and recommendations. At the time of responding to the draft audit, the Board itself has not had the opportunity to meet and discuss. We will discuss the final report with the Board upon release and whether amendments to the BSCC regulations are warranted.
Sincerely,
KATHLEEN T. HOWARD
Executive Director
Comments
California STATE AUDITOR’S COMMENTS ON THE RESPONSE FROM THE BOARD OF STATE AND COMMUNITY CORRECTIONS
To provide clarity and perspective, we are commenting on the BSCC’s response to our audit. The numbers below correspond to the numbers we have placed in the margin of its response. Rather than comment on all of the individual areas of its response that we believe are deficient or misleading, we have summarized our comments according to the respective sections in its response.
①We stand by our recommendation that the Legislature should amend state law to require sheriff’s departments with larger jail populations to have mental health professionals perform mental health evaluations at intake. We based this recommendation on the problems identified in our review of the San Diego Sheriff’s Department and the variation of policies among the three comparable counties. In some of the cases we reviewed, the Sheriff’s Department did not promptly and properly identify individuals’ mental health needs because mental health professionals generally do not participate in its intake health screenings. In contrast, we noted that one county has adopted more robust intake screening practices. For example, Riverside Sheriff’s Department policy requires that a mental health clinician evaluate every individual before being housed, which could help to more effectively identify mental health needs early.
Further, BSCC infers our recommendation is to establish lesser standards of mental health staffing for smaller counties. On the contrary, we did not propose any changes to these standards for smaller counties, but instead recommend that BSCC should raise the standard for the larger counties.
②BSCC suggests that counties electing to have more robust safety checks policies does not mean that its minimum standards are inadequate. We disagree. BSCC’s standards do not describe the actions that constitute an adequate safety check. Instead, the standards simply state that safety checks must be conducted at least hourly through direct visual observation of all inmates and that observation through a video camera alone is not sufficient. Consequently, we found the four counties we reviewed based their policies on different interpretations of this standard. Further, based on our review of video of San Diego Sheriff’s Department, we observed multiple instances of sworn staff who spent no more than one second glancing into an individual’s cell, sometimes without breaking stride as they walked through the housing module. Staff later discovered individuals unresponsive in their cells, some with signs of having died several hours earlier.
Further, we concluded that sworn staff conducted safety checks inadequately in part because of weaknesses in the San Diego Sheriff’s Department’s policy. In particular, its safety check policy does not require sworn staff to determine whether individuals are alive and well by taking steps such as by observing the rise and fall of their chest. We recognize that acquiring proof of life in some situations is difficult and that waking up incarcerated individuals every hour could be detrimental to their well‑being. However, a safety check that does not involve any meaningful observation of an individual is ineffective and inadequate.
Moreover, BSCC asserts that our report references a CDCR policy that merely serves as instructions for a proper population count. However, CDCR’s policy is a requirement for an hourly check that is equivalent to what BSCC refers to as a safety check. We revised the report text here to be more explicit that the CDCR policy is for an hourly check of incarcerated individuals.
Finally, BSCC states that its proposed regulations exceed the standards in other states and are aligned with best practices. However, it falls short of the State’s best practice. For example, CDCR requires its staff during its hourly checks to count a living, breathing individual whom they see in person. BSCC’s proposed regulations are insufficient because, it fails to specify that a safety check must include verifying that an individual is alive, which is essential to ensuring the safety of incarcerated individuals across the State.
③Our recommendation to increase the required number of continuing education hours for local correctional officers is based on concerns observed in our review of how San Diego Sheriff’s Department sworn staff responded to medical, mental health, and safety needs. Further, given the increase in the annual number of in‑custody deaths across the State from 130 in 2006 to 156 in 2020, improving statewide standards related to health and safety and training requirements is essential to ensuring the health and safety of incarcerated individuals.
BSCC’s statement that its standards require 21 hours of behavioral health training is misleading because this training pertains only to initial hires. The point of continuing education is to provide local correctional officers with ongoing training to expand their foundation of knowledge to promote health and safety within the jails and to stay up‑to‑date on new information that would help in that effort.
We stand by our conclusion that the continuing education requirements are inconsistent. BSCC’s required training hours for sworn staff working in local detention facilities do not align with their standards for similar positions. Requiring fewer hours for adult corrections personnel does not make sense when thousands of individuals are incarcerated in these facilities and the number of individuals who have died has increased over the past 15 years. Further, BSCC does not require that any of the annual training cover topics pertaining to mental health, even though best practices suggest staff should receive at least four hours of mental health training annually. Increasing the number of training hours to align with similar professions, including mandating mental health training hours, could allow sheriff’s departments to better protect and keep incarcerated individuals safe.
Similar to our recommendation for having mental health professionals perform mental health assessments at intake, BSCC should increase the required continuing education hours for counties that house the majority of individuals in the county jail systems. Moreover, contrary to BSCC’s assertion, we did not propose any changes to these standards for smaller counties but instead recommend that it should raise the standard for the larger counties.
Citizens’ Law Enforcement Review Board
January 14, 2022
Michael S. Tilden, CPA
Acting California State Auditor
621 Capitol Mall, Suite 1200
Sacramento, CA 95814
RE: Response to California State Auditor’s Draft Report 2021-109: San Diego County Sheriff’s Department
Dear Mr. Tilden:
The Citizens’ Law Enforcement Review Board (CLERB) welcomes the opportunity and has authorized me to respond to the California State Auditor’s (CSA) draft report, titled, “San Diego County Sheriff’s Department,” in which analyses and recommendations about CLERB were documented.
CLERB’s responses to your specific recommendations, of which the CSA proposes completion by May 2022, are set forth below:
- Recommendation One: Discuss and modify its current agreement with the Sheriff’s Department and the labor organization to allow CLERB’s investigators to conduct independent interviews of Sheriff’s Department sworn staff.
①Agree. In the last quarter of 2021, the current CLERB Executive Officer (EO), the Deputy Sheriff’s Association (DSA) President, DSA Counsel, and CLERB Outside Counsel met to discuss the agreement for the purpose of conducting in-person interviews with Sheriff’s Department sworn staff. Additional discussions are forthcoming.
- Recommendation Two: Develop a comprehensive training manual for its investigators that outlines standard procedures for investigations. The manual should include a specific section dedicated to investigations of in-custody deaths, including guidance for evaluating the circumstances leading up to an in-custody death, such as the decedent’s mental health history and the appropriateness of the decedent’s housing assignment.
Agree. While it is true that there does not exist a physical stand-alone comprehensive training manual, new CLERB Special Investigators are currently provided with copies of CLERB’s internal documented policies and procedures (P&P), database user guide, investigative report templates, and a comprehensive resource manual containing the following materials:
- County structure
- CLERB historical perspective
- County Charter, Section 606
- County Administrative Code, Section 340
- CLERB Rules and Regulations
- Civil Service Commission Rule XV
- Case Law Including and impacting CLERB
- Public Safety Officer Procedural Bill of Rights (POBOR)
- Statutes Pertaining to Peace Officer Records
- San Diego County Grand Jury Reports Pertaining to CLERB
- Ralph M. Brown Act
- San Diego County Operational Plan Pertaining to CLER
The P&P, user guide, report templates, and topics contained within the resource manual are thoroughly discussed and reviewed with the trainee during his/her training program. These materials will be incorporated into the referenced stand-alone training manual, which will also include evaluations of a trainee’s performance and documentation as to his/her progress, or lack thereof.
①The comprehensive training manual will also include a specific section dedicated to investigations of in-custody deaths. Despite the current absence of the stand-alone training manual, trainees are specifically instructed, during their training programs, to evaluate the circumstances leading up to an in-custody death, and to include a review of the decedent’s mental health history and the appropriateness of the decedent’s housing assignment. In addition to these critical topics, trainees are also instructed to evaluate the timeliness and thoroughness of welfare checks conducted on the decedent by deputies and assess whether deputies appropriately determined that a life-threatening emergency existed and responded accordingly.
- Recommendation Three: Create policies and procedures to require its investigators to finish casework on in-custody death investigations within three months of receiving the homicide investigation file. These policies and procedures should also require investigators to attempt to independently verify any information they receive from the Sheriff’s Department; to thoroughly review deputy statements and reports from the homicide investigation file; and to request interviews with relevant detentions staff and other witnesses in all instances where they identify discrepancies or missing information.
②Agree. The current CLERB EO directed that the completion of in-custody death investigations within three months of receiving the homicide investigation file would take effect when CLERB filled its third and final CLERB Special Investigator vacancy. As that vacancy was filled on January 10, 2022, this mandate will now be incorporated into existing CLERB Policy #300.5, entitled, “Death Investigations.” The independent verification of information received from the Sheriff’s Department and the already existing practices of thoroughly reviewing deputy statements and reports from the homicide file and requesting interviews from witnesses, when contact information is known and time constraints do not exist, will be codified into P&P.
- Recommendation Four: CLERB should revise its rules and regulations to include prioritization criteria for investigating in-custody deaths above all other investigations.
③Agree. The Policy Statement in CLERB Policy #300.5, entitled, “Death Investigations,” issued by the current EO on August 27, 2021, indicates that it is the policy of CLERB “that death cases will take priority over any other CLERB case.” During the current EO’s previous tenure as EO from June 2017 to September 2018, he implemented this practice, and all death cases were made the highest priority. During his absence from September 2018 to November 2020, for unknown reasons, death cases were not handled as the highest priority. To ensure that the investigation of death cases remains the highest priority after any future executive management changes, a five-tiered case categorization system should be documented in the Rules and Regulations, with “Category I” being the highest priority and “Category V” being the lowest priority. Death investigations should be classified as “Category I.”
- Recommendation Five: CLERB should revise its rules and regulations to include clarification that its investigations of in-custody deaths includes those classified as natural deaths.
Agree. During the current EO’s previous tenure as EO from June 2017 to September 2018, he implemented the practice of invoking CLERB’s jurisdiction on every in-custody-related death, to include those that the Medical Examiner’s Office determined to be due to natural causes. To ensure that the investigation of all in-custody-related deaths continue after any future executive management changes, CLERB’s Rules and Regulations should not only be revised to clarify that in-custody natural deaths are within CLERB’s jurisdiction, but that all deaths occurring in the custody of the Sheriff’s Department or related to instances or occurrences within the Sheriff’s Department detention facilities are within CLERB’s jurisdiction. As these proposed Rules and Regulations changes may first require the amendment of the County Charter and/or the County Administrative Code, the CLERB EO will need to work with CLERB’s legal counsel to pursue implementation of this recommendation.
- Recommendation Six: CLERB should perform an analysis of overall trends related to these deaths, including demographic information, and determine whether the trends suggest deficiencies in the Sheriff’s Department’s policies and procedures. It should also identify policy recommendations for improving the safety of individuals in the Sheriff’s Department’s custody. CLERB should include these trends and analysis in its annual reports starting with its 2021 report.
Agree. The current EO has prioritized in-custody death investigations and the analysis of overall trends related to the deaths, to include demographic information. Upon his return to CLERB in late 2019, he authored CLERB’s 2020 Annual Report and provided a detailed breakdown of the 18 death cases CLERB opened in 2019 and the 15 death cases CLERB opened in 2020 (this breakdown is documented on pages 10 and 11 of the Annual Report). In addition, he provided a list of all death cases opened by CLERB in 2019 and 2020 and closed by CLERB in 2019 and 2020. The list included the decedent’s name, type of death, detention facility/patrol area, and cause of death (this list is documented on pages 28 thru 33 of the Annual Report). After the finalization of the 2020 Annual Report and its presentation to the Board of Supervisors, the current EO committed to expanding the reporting to include an analysis of overall trends related to deaths, including demographic information, in the 2021 Annual Report.
④CLERB has averaged 10 policy recommendations per calendar year over the past three years. The majority of the recommendations pertained to the Sheriff’s Department’s detention facilities. Finally, it should be noted that CLERB will, for the first time in its 30-plus year history, conduct detention facility inspections in 2022. The scope of the inspections will be specifically tailored to each detention facility based upon the complaints received from its inmates, great bodily injuries received from deputies’ uses of force, and deaths occurring at or stemming from incarceration within it.
We look forward to updating the CSA on progress made within six months. Our commitment to continuing the proactivity started at the end of 2020 to improve upon the invaluable civilian oversight role we provide to the public, the Sheriff’s Department, and the County is unwavering. The implementation of the CSA recommendations will assist with CLERB’s provision of independent, timely, full, and thorough investigations into in-custody deaths which may, in turn, prevent future deaths.
Thank you for the opportunity to provide this response and for the professionalism and courtesy shown by your staff throughout this process.
Sincerely,
Paul R. Parker III
Executive Officer, CLERB
cc: CLERB Members
Shiri Hoffman and Aurelia Razo, Senior Deputies County Counsel
James Sandler; Sandler, Lasry, Laube, Byer & Valdez LLP
Comments
CALIFORNIA STATE AUDITOR’S COMMENTS ON THE RESPONSE FROM THE CITIZENS’ LAW ENFORCEMENT REVIEW BOARD
To provide clarity and perspective, we are commenting on CLERB’s response to our audit. The numbers below correspond to the numbers we have placed in the margin of its response.
①Although CLERB states that it provides various materials and training to its staff, we found some cases in which CLERB’s investigators did not appear to consider all the circumstances leading up to the deaths, did not examine all the relevant Sheriff’s Department policies, and did not follow up on discrepancies they discovered in the course of their investigations. Accordingly, our recommendation is for CLERB to develop a comprehensive training manual to ensure that its investigations are complete and thorough.
②Contrary to its response, we found that CLERB did not always independently verify information from the Sheriff’s Department. As we note, when investigating an altercation between two cellmates resulted in the death of one of the individuals, we found the CLERB investigator did not appear to scrutinize or independently verify evidence that could have sufficiently determined whether the Sheriff’s Department’s actions violated policies or procedures. Further, we question CLERB’s statement that it thoroughly verifies deputies’ statements. As we state on page 43, CLERB did not independently interview staff from the Sheriff’s Department in any of the six cases we reviewed.
③Although CLERB recently added policies and procedures establishing its prioritization of death cases over all other cases, it did not do so until August 2021. Moreover, because policies can easily be changed when leadership changes, it is important that CLERB include requirements in its rules and regulations for how it prioritizes cases.
④CLERB’s statement that it has averaged 10 policy recommendations per calendar year is primarily referring to the recommendations it makes based on individual cases. CLERB generally makes recommendations based on individual cases rather than on trends it identifies through analysis of its investigations. Making recommendations based on trends could help resolve more systemic concerns at the Sheriff’s Department.
California Department of Justice
January 14, 2022
Michael S. Tilden, CPA California State Auditor
621 Capitol Mall, Suite 1200
Sacramento, CA 95814
Re: Draft Audit Report - California State Auditor Report 2021-109; San Diego County Sheriff’s Department –Inmate Custody Death
Dear Mr. Tilden,
The Department of Justice (DOJ) appreciates the opportunity to review the above-mentioned draft audit report.
The audit recommends that to ensure that all sheriff’s departments accurately report deaths that occur from incidents or conditions in county jails, the Legislature should amend state law to require sheriff’s departments to report to the attorney general individuals who are released from custody after being transported directly to a hospital or similar medical facility, and subsequently dies in the facility. It should also amend state law to require sheriff’s departments to provide the attorney general with all facts concerning the death, such as the cause and manner.”
DOJ supports increased transparency of data reporting. As the audit notes, there is currently no statutory requirement in place to require sheriff’s departments to report individuals released from custody after being transported directly to a medical facility who subsequently dies in the facility. Express authority from the Legislature and funding is needed to implement this new data reporting recommendation. Furthermore, should the Legislature implement the recommendation requiring sheriff’s department disclose the cause and manner of the death, DOJ will work with the Legislature to ensure that any policies comply with all applicable confidentiality laws.
If you have any questions or concerns regarding this matter, you may contact me at the telephone number listed above.
Sincerely,
2022.01.14 16:46:08
-08'00'
Joe Dominic, Chief
California Justice Information Services Division
For ROB BONTA
Attorney General
cc: Venus D. Johnson, Chief Deputy Attorney General
Chris Prasad, CPA, Director, Office of Program Oversight and Accountability
San Diego County Sheriff's Department
January 14, 2022
Ms. Elaine M. Howle
California State Auditor
621 Capitol Mall, Suite 1200
Sacramento, California 95814
State Auditor Howle:
Attached please find the response from the San Diego County Sheriff's Department in reference to your draft audit report on the San Diego County jails.
Sincerely,
William D. Gore, Sheriff
①THE CALIFORNIA STATE AUDITOR DID NOT PROVIDE SUFFICIENT OPPORTUNITY FOR THE SAN DIEGO COUNTY SHERIFF'S DEPARTMENT TO REVIEW AND RESPOND TO THE AUDIT
② the San Diego Sheriff's Department received a draft copy of the State Auditor's Report 2021-109 for the stated purpose of allowing the Department to review and respond to the audit. The Sheriff's Department was afforded less than five (5) days to review and respond to the draft report, as the audit was received late in the morning on Monday and the response was due back by 5:00 p.m. on Friday.
③The 2018 revision of Government Auditing Standards, commonly referred to as generally accepted government auditing standards (GAGAS), is effective for performance audits beginning on or after July 1, 2019, such as the instant engagement. GAGAS section 9.50 provides that "Auditors should obtain and report the views of responsible officials of the audited entity concerning the findings, conclusions, and recommendations in the audit report, as well as any planned corrective actions." The highly redacted version of the draft report, coupled with the short time afforded for review and response, and the lack of supporting documentation, makes it difficult for the Sheriff's Department, as the audited entity, to submit a meaningful, comprehensive response to the draft report.
①Accordingly, the Sheriff's Department reserves the right to submit a more comprehensive response after the final report and any supporting documentation and information are published, as none of the supporting documentation and information was included with the draft report transmission.
Introduction
The gravity and seriousness of in-custody deaths and the importance of identifying and improving deficiencies when they occur is not lost on the San Diego Sheriff's Department. We have been transparent in our response to the Joint Legislative Audit Committee's recommendation that the California State Auditor review in-custody deaths in San Diego County. During the audit, we cooperated fully and provided complete access to our records, facilities, and personnel.
④ ⑤The Sheriff's Department was pleased to see that the auditors' findings confirm that the Department's policies and procedures align with the minimum standards established through state law and other applicable guidance. That said, while the Sheriff's Department appreciates the work and recommendations of the auditors, the Department maintains concerns regarding the findings, as well as the conclusions and recommendations contained in the draft report and the way the audit was conducted.
⑥I. The Audit Failed to Conform with Generally Accepted Government Auditing Standards
California Government Code section 8546.1(c) requires that the State Auditor "complete any audit in a timely manner and pursuant to the 'Government Auditing Standards' published by the Comptroller General of the United States." While the State Auditor recognizes that the instant engagement is undertaken pursuant to GAGAS, it failed to conform to the requisite standards.
⑥A. The auditors failed to comply with reporting standards for performance audits
GAGAS section 9.03 provides, "[w]hen auditors comply with all applicable GAGAS requirements, they should use the following language, which represents an unmodified GAGAS compliance statement, in the audit report to indicate that they conducted the audit in accordance with GAGAS:
We conducted this performance audit in accordance with generally accepted government auditing standards. Those standards require that we plan and perform the audit to obtain sufficient, appropriate evidence to provide a reasonable basis for our findings and conclusions based on our audit objectives. We believe that the evidence obtained provides a reasonable basis for our findings and conclusions based on our audit objectives.
The section 9.03 compliance statement is notably absent from the draft report.
In the event auditors do not comply with all applicable GAGAS requirements, section 9.05 provides, "they should include a modified GAGAS compliance statement in the audit report. For performance audits, auditors should use a statement that includes either (1) the language in paragraph 9.03, modified to indicate the requirements that were not followed, or (2) language indicating that the auditors did not follow GAGAS."
Similarly, a section 9.05 alternate compliance statement is also absent from the draft report.
⑥B. The auditors have declined to adopt the GAGAS report quality elements of accurate, objective, complete, convincing, and timely in developing and writing the audit report
Chapter 9 of the GAGAS addresses the reporting standards for performance audits such as the instant engagement. GAGAS section 9.17 provides that “[t]he auditor may use the report quality elements of accurate, objective, complete, convincing, clear, concise, and timely when developing and writing the audit report as the subject permits.” For purposes of the instant engagement, the auditors failed to adopt the report quality elements of accurate, objective, complete, convincing and timely in developing and writing the audit report.
⑦a. Accuracy
Section 9.17(a) regarding report quality element “Accurate” states, in pertinent part, “[a]n accurate report is supported by sufficient, appropriate evidence with key facts, figures, and findings being traceable to the audit evidence. Reports that are fact-based, with a clear statement of sources, methods, and assumptions so that report users can judge how much weight to give the evidence reported, assist in achieving accuracy.”
Consistent with this standard, the Auditor makes recommendations to the legislature for policy revisions "to better align with best practices, as follows." There is no data or evidence cited to support the best practices recommendations. Data and evidence-based approaches to medical, mental health and correctional care policies are necessary to ensure the best health and safety outcomes for incarcerated individuals. In other sections, the auditor states "[r]eports and studies related to mental health indicate that…" There is no reference to which studies and reports are being relied upon for the assertions.
The audit states, "that deficiencies in the Sheriff's Department's policies and practices related to intake screenings, medical and mental health care, safety checks, and responses to emergencies likely contributed to these deaths," the report is devoid of any evidence that the deaths were cause by a failure of the department's policies or practices.
While no death is acceptable, the Sheriff recognizes that some incarcerated individuals have pre-existing conditions, age or other maladies which lead to natural death. These deaths made up nearly half of all the deaths that occurred during the 15-year audit period. The report does not explain if a failure on the part of the department caused the death or if those individuals could have died in the community from the same pre-existing condition.
The Sheriff's Department has implemented extensive programs, training, and policies to prevent suicide in the jails. The jails disproportionately house individuals suffering from mental illness, and substance use disorder. The identification of individuals who wish to do themselves harm is one key to prevention and removing the ability to commit self-harm is the second. Individuals bent on harming themselves creates obstacles to identification and prevention. Similarly, substance use disorder is an enormous driver for behavior. It could be argued that in-custody individuals are even more driven to use substances to alleviate the strain and monotony of incarceration. The Sheriff's Department has created extensive layers and policies to interdict and prevent contraband from being smuggled into the jail system. We have instituted the use of naloxone to save lives when someone is successful in circumventing those interdiction efforts. While the Sheriff's Department can always do better, the audit does little to document or provide context for those efforts and the complexity of keeping individuals safe from themselves.
⑥b. Objectivity
Section 9.17(b) regarding report quality element “Objective” states, in pertinent part, “[o]bjective means that the presentation of the report is balanced in content and tone. A report’s credibility is significantly enhanced when it presents evidence in an unbiased manner and in the proper context. This means presenting the audit results impartially and fairly. The tone of reports may encourage decision makers to act on the auditors’ findings and recommendations. This balanced tone can be achieved when reports present sufficient, appropriate evidence to support conclusions while refraining from using adjectives or adverbs that characterize evidence in a way that implies criticism or unsupported conclusions.” (Emphasis added).
Despite the fact that section 9.17(b) specifically counsels against using such adjectives and adverbs, the draft report is replete with such unsupported criticism (e.g. "likely contributed to the deaths," “inadequate response to deaths,” "might have placed this individual," “lack of effective independent oversight,” “meaningful changes,” “meaningful corrective action,” “few substantive steps,” “have not consistently led to significant corrective action,” “failure to adequately prevent the deaths,” "could help," and "could be useful"). Use of such terms, in contravention of the GAGAS guidance, calls into question and undercuts the objectivity of the engagement and the resulting instant report.
Section 9.17(b) goes on to provide, “[a]udit reports are more objective when they demonstrate that the work has been performed by professional, unbiased, independent, and knowledgeable personnel.” (Emphasis added). As discussed more fully below, the auditors lack the requisite knowledge, skills and abilities necessary to competently conduct the instant engagement.
⑥c. Completeness
Section 9.17(c) regarding the report quality element “Complete” states, in pertinent part, “complete means that the report contains sufficient, appropriate evidence needed to satisfy the audit objectives and promote an understanding of the matters reported. It also means the report states evidence and findings without omission of significant relevant information related to the audit objectives. Providing report users with an understanding means providing perspective on the extent and significance of reported findings, such as the frequency of occurrence relative to the number of cases or transactions tested and the relationship of the findings to the entity’s operations.” (Emphasis added).
⑧The auditors’ summary of the event outlined in Case Example 4 illustrates the omission of significant relevant information in an effort to paint a picture that deputies stood idly by while CPR was medically indicated for the incarcerated individual. Based on our review of Case Example 4, we believe the auditors are referring to Sheriff’s case number
The auditors' description of the event depicted in the chart above misleads the reader, is an example of the lack of completeness and objectivity that is present in the draft report and fails to meet the report quality elements outlined in GAGAS sections 9.17(b) and 9.17(c).
⑥d. Convincing
Section 9.17(d) regarding report quality element “Convincing” states, in pertinent part, "convincing means that the audit results are responsive to the audit objectives, that the findings are presented persuasively, and that the conclusions and recommendations flow logically from the facts presented. The validity of the findings, the reasonableness of the conclusions, and the benefit of implementing the recommendations are more convincing when supported by sufficient, appropriate evidence.”
While the draft report speaks to best practices, the draft contains no such policies, best practices, or sample language, nor the jurisdiction(s) where such best practices were or are being implemented. As discussed in Section C. below, while good intentioned, best practices suggested by auditors without the requisite knowledge, skills, and abilities, may violate the constitutional rights of incarcerated individuals, cause harm to the mental health of incarcerated individuals and ultimately result in increased liability to the County. By not including copies of the best practices referenced throughout the draft report, it is difficult for the Sheriff’s Department to ascertain whether the suggested best practices comport with state law, Title 15 regulations and the constitutional rights guaranteed to incarcerated individuals.
③The draft report does contain one table (Table 2) with excerpts of safety check policies, however, while excerpts from the BSCC policy and the Sheriff's Department policy are unredacted, the policies and names of the three other entities are redacted in their entirety.
③i. The Auditor Improperly Redacted Public Documents and Refused to Provide the Documents to the Sheriff's Department Necessary for the Department to Provide a Meaningful Response
For purposes of an engagement under GAGAS, the terms "auditee" and "audited entity" are interchangeable. GAGAS section 1.27(e) defines an "audited entity" as "[t]he entity that is subject to a GAGAS engagement, whether that engagement is a financial audit, attestation engagement, review of financial statements, or performance audit."
The Joint Legislative Audit Committee (JLAC) charged the auditor with conducting an audit of the San Diego Sheriff's Department and the County of San Diego Citizens Law Enforcement Review Board (CLERB). The auditor confirmed the scope of its engagement in the document entitled 2021-109 Audit Scope and Objectives, identifying the audited entities as the San Diego County Sheriff's Department and the CLERB. No other agencies were identified as audited entities (or auditees).
⑨Based upon the GAGAS standards, and the JLAC referral, Alameda, Orange County, and Riverside are not auditees. However, even if they were, the information relied upon should have been given to the Sheriff's Department, as the auditee, to respond to the draft report, because it is public information.
The Sheriff's Department must meet Title 15 standards for its detention facilities, as do other local detention facilities throughout the State of California. For the redacted policy excerpts to be relevant to the auditors' engagement, the redacted excerpts are presumably from other law enforcement agencies in the state.
Policies of a California law enforcement agency are public record. Senate Bill 978 (SB 978) added section 13650 to the Government Code, which requires "…each local law enforcement agency shall conspicuously post on their Internet Web sites all current standards, policies, practices, operating procedures, and education and training materials that would otherwise be available to the public if a request was made pursuant to the California Public Records Act (Chapter 3.5 (commencing with Section 6250) of Division 7 of Title 1 of the Government Code)." As such, each California law enforcement agency is required to publicly post, on its website, all its policies and procedures, such as its detention facilities safety check policy.
⑩It is well settled that a governmental agency cannot shield records that are subject to public disclosure simply by putting those publicly available records in a file it stamps "confidential." Therefore, the auditor should have provided the policies which it relied on in creating its report.
⑩Similarly, it was improper for the auditor to redact and withhold from disclosure settlement information it obtained, admittedly, from publicly available court documents regarding the three selected counties it designated as comparable counties.
e. Timeliness
Section 9.17(g) regarding report quality element “Timely” states, in pertinent part, “[t]o be of maximum use, providing relevant evidence in time to respond to officials of the audited entity, legislative officials, and other users’ legitimate needs is the auditors’ goal. Likewise, the evidence provided in the report is more helpful if it is current.”
⑪While it is certainly helpful from a historical perspective to discuss changes in policies or procedures, it is unclear whether the auditors’ findings and conclusions are based on the policies and procedures as they existed at the time of the incident under review or present-day policies and procedures. For example, the draft report states, “...although the Sheriff’s Department's policy indicates that a nurse should conduct a face-to-face appraisal with an incarcerated individual within 24 hours of a mental health care request to determine the urgency of that request, it has not always had this policy.” The Sheriff’s Department believes this change in policy was a positive step, but it is unclear whether the auditors’ findings and recommendations are based on current policies and procedures, or policies and procedures that were in place at the time of the incident under review.
⑥c. The Auditors' Lack of Requisite Knowledge, Skills and Abilities Necessary to Conduct the Instant Engagement Raise Ethical and Competence Issues under the Generally Accepted Government Auditing Standards
Chapter 3 of the GAGAS sets forth fundamental ethical principles for auditors in the government environment.
Section 3.04 relating to ethical principles provides that "[p]erforming audit work in accordance with ethical principles is a matter of personal and organizational responsibility." The section goes on to clearly state that ethical principles apply in "taking on only work that the audit organization is competent to perform…"
To ensure that an audited entity is afforded a fair, unbiased and meaningful audit, Chapter 4 of the GAGAS requires that the auditors collectively possess the competence needed to address the engagement objectives and perform their work in accordance with GAGAS. The knowledge, skills, and abilities needed when conducting an engagement in accordance with GAGAS include the understanding necessary to proficiently apply a. GAGAS; b. standards, statutory requirements, regulations, criteria, and guidance applicable to auditing or the objectives for the engagement(s) being conducted; and c. techniques, tools, and guidance related to professional expertise applicable to the work being performed. (Emphasis added). (GAGAS section 4.07).
GAGAS section 4.08 provides, "[a]chieving the knowledge, skills, and abilities needed to conduct a GAGAS engagement may include: a. having prior experience in the subject matter or type of engagement; b. completing [continuing professional education] related to the subject matter or type of engagement; and c. obtaining degrees or certifications relevant to the subject matter or type of engagement."
The instant engagement requires knowledge, skills, and abilities regarding varied areas in the detentions or corrections environment including, but not limited to, detentions custodial operations, detentions medical services and detentions mental health functions.
This knowledge is so important that state law requires that a deputy complete an introductory training course by the Commission on Peace Officer Standards and Training, additional training by the Board of State and Community Corrections, and specialized training for custodial personnel of local detention facilities pursuant to Title 15 of the California Code of Regulations. In addition to this initial 16 weeks of academy training, deputies are next assigned to phase training where they are paired up with seasoned training officers before they can function on their own. After these initial academy and training phases, detentions deputies are required by state law to complete a minimum of 24 hours of annual training to maintain their proficiency and certification.
The professional qualifications necessary for detentions medical doctors, registered nurses, licensed vocational nurses, and mental health clinicians must satisfy not only the educational requirements of their field which often includes many years of studies, and successfully passing the tests required by their licensing authority, but also continuing professional education in order to maintain their license or certification.
②Additionally, the field of corrections is a highly regulated field of law comprised of state and federal Constitutional standards and laws, as well as case law issued by the U.S. Supreme Court, federal, and state courts. Changes in department policies can impact an inmate's constitutional rights, and a lack of knowledge regarding correctional law can lead to flawed policies and constitutional violations.
②The requisite knowledge, skills, and abilities necessary to render an informed opinion regarding detentions custodial operations would be satisfied by either an auditor, or a specialist"Some engagements may necessitate the use of specialized techniques or methods that call for the skills of specialists. Specialists do not include individuals with special skill or knowledge related to specialized areas within the field of accounting or auditing, such as income taxation and information technology. Such individuals are considered auditors." (Emphasis added). GAGAS section 4.13. "The competence and qualifications of specialists significantly affect whether their work will be adequate for the engagement team’s purposes and will meet GAGAS requirements. Competence of specialists relates to the nature and level of expertise. Qualifications of specialists relate to their professional certifications, reputations, and previous work in the subject matter. Other relevant factors include the ability of specialists to exercise competence in the circumstances of the engagement and the effects that bias, conflict of interest, or the influence of others may have on the specialists’ professional judgment." GAGAS section 4.14. "Sources that may inform the auditors’ assessment of the competence and professional qualifications of a specialist include the following: a. the professional certification, license, or other recognition of the competence of the specialist in his or her field, as appropriate; b. the reputation and standing of the specialist in the views of peers and others familiar with the specialist’s capability or performance; c. the specialist’s experience and previous work in the subject matter; d. the auditors’ assessment of the specialist’s knowledge and qualification based on prior experience in using the specialist’s work; e. the specialist’s knowledge of any technical performance standards or other professional or industry requirements in the specialist’s field (for example, ethical standards and other membership requirements of a professional body or industry association, accreditation standards of a licensing body, or requirements imposed by law or regulation); f. the knowledge of the specialist with respect to relevant auditing standards; and g. the assessment of unexpected events, changes in conditions, or the evidence obtained from the results of engagement procedures that indicate it may be necessary to reconsider the initial evaluation of the competence and qualifications of a specialist as the engagement progresses." (Emphasis added). GAGAS section 4.15. engaged to assist the audit team, who was certified by the State of California, Bureau of State and Community Corrections (BSCC), Standards and Trainings for Corrections (STC). it does not appear that any of the audit team members possess such training or certification.
It is further generally recognized that the function of providing medical services in the correctional setting is different than in a public setting. According to the American Academy of Family Physicians, “[i]nmates in correctional facilities have significantly higher rates of disease than the general population, and … tend[] to suffer in greater numbers from infectious disease, mental health problems, and substance use and addiction.” The requisite knowledge, skills, and abilities necessary to render an informed opinion regarding detentions medical services would be satisfied by either an auditor, or a specialist engaged to assist the audit team, who is, or was, a medical doctor or registered nurse in a detentions or corrections environment. In our discussions with the auditors, it does not appear that any of the audit team members possess such training or experience.
②Similarly, the requisite knowledge, skills, and abilities necessary to render an informed opinion regarding detentions mental health functions would be satisfied by either an auditor, or a specialist engaged to assist the audit team, who is or was a qualified mental health provider (QMHP) or mental health clinician (MHC) in a detentions or corrections environment. it does not appear that any of the audit team members possess such training or experience.
By way of example, the Sheriff's Department was previously reviewed by subject matter experts who possessed the requisite knowledge, skills, and abilities necessary for the scope of their engagement. One review was conducted by Mr. Lindsey HayesLindsay M. Hayes is a Project Director of the National Center on Institutions and Alternatives (NCIA) and is nationally recognized as an expert in the field of suicide prevention within jails, prisons, and juvenile facilities. He has been a consultant to the U.S. Justice Department's Civil Rights Division in its investigations of conditions of confinement in both adult and juvenile correctional facilities throughout the country. He has also been appointed as a Federal Court Monitor in the monitoring of suicide prevention practices in several adult and juvenile correctional systems under court jurisdiction. He has served as an expert witness/consultant in litigation cases involving the suicide of incarcerated individuals, and his expertise has allowed him to conduct training seminars and assessments of adult and juvenile suicide prevention practices within correctional facilities throughout the country. Hayes is a published author with over 60 publications in the area of suicide prevention within adult and juvenile correctional facilities and has conducted the only five national studies of jail, prison, and juvenile suicide (And Darkness Closes In…National Study of Jail Suicides in 1981, National Study of Jail Suicides: Seven Years Later in 1988, Prison Suicide: An Overview and Guide to Prevention in 1995, Juvenile Suicide in Confinement: A National Survey in 2004, and National Study of Jail Suicide: 20 Years Later in 2009). Hayes has reviewed over 3,000 cases of suicide in jail, prison, and juvenile facilities throughout the country over the past 30 years. He was awarded the National Commission on Correctional Health Care's Award of Excellence in 2001, for his contribution in the field of suicide prevention in correctional facilities. His work has been cited in several state and national correctional health care standards, and numerous suicide prevention training curricula, including the National Institute of Correction (NIC). , the other review was conducted by the National Commission on Correctional Health Care (NCCHC)The National Commission on Correctional Health Care (NCCHC) is a non-profit 501(c)(3) organization whose mission is to improve the quality of health care in jails, prisons, and juvenile confinement facilities. The NCCHC establishes standards for health services in correctional facilities, produces resource publications, conducts educational conferences, offers a certification for correctional health professionals and a voluntary accreditation program for institutions that meet their standards. The NCCHC is supported by numerous major national organizations in the fields of health, law, and corrections. The NCCHC has a multidisciplinary governing structure, which addresses the complexities of correctional health care, and whose standards for health services in correctional facilities is widely recognized. NCCHC's standards address areas of care and treatment, health records, administration, personnel and medical-legal issues; and offer voluntary health services accreditation based on its standards. NCCHC also hold conferences with educational programs that address topics such as mental health and substance abuse services. The NCCHC publishes periodicals such as the Journal of Correctional Health Care and CorrectCare, which are the leading periodicals in this field. The NCCHC offers consultation and assistances to facilities with issues preparing for accreditation, developing policies and procedures, and assessing alternative solutions to problems. .
In order to demonstrate that the auditors assigned to this engagement possessed the requisite knowledge, skills, and abilities in detentions custodial operations, detentions medical services and detentions mental health functions, as required by GAGAS, the Sheriff's Department requests that the State Auditor include in its final report the curricula vitae for each auditor and specialist assigned to the instant engagement, including any relevant continuing professional education regarding the subject matter of the engagement.
II. The San Diego County Sheriff’s Department Has Taken Appropriate and Reasonable Measures to Prevent and Respond to Deaths of Individuals in Custody
⑦a. The Auditor's Conclusion That the In-Custody Deaths Were the Result of Inadequate Medical Care is Misleading
⑦While the first sentence of the draft report begins with the recognition that the Sheriff's Department is responsible for providing medical care to individuals in its custody, the next sentence goes on to state: "Nonetheless, from 2006 through 2020, 185 people died in San Diego County jails – more than in nearly any other county across the state." The transition from the statement that the Sheriff's Department is responsible for providing adequate medical care to the statement that "nonetheless" 185 people died in San Diego County jails is misleading and implies that the deaths were the result of inadequate medical care.
②The draft report does not identify which deaths were the result of "inadequate" medical care. Natural deaths comprise nearly half, the highest percentage, of in-custody deaths identified by the auditors. the draft report does not identify what medical care was inadequate, nor does it identify what medical care the Sheriff's Department should have provided that would have avoided individuals from dying of natural causes, such as heart disease, cancer, chronic lower respiratory disease (COPD, emphysema, chronic bronchitis), and stroke. Just as individuals with these conditions die from their conditions in the community setting, incarcerated individuals with these conditions often die from their conditions while in custody, not as the result of incarceration or the medical care they receive while incarcerated but as a natural and expected progression of their condition.
Similarly, while accidental deaths account for 31 of the total in-custody deaths during the audited period, the draft report does not identify any medical care that was "inadequate" resulting in an individual's death. As the auditors are aware, most of the accidental deaths were the result of individuals overdosing on drugs, not due to "inadequate" medical care. In response to the opioid epidemic, the San Diego Sheriff's Department was one of the first departments in the state to equip not only its detentions medical staff but also detentions deputies with NARCAN® (naloxone HCL) nasal spray to combat the surge in opioid overdoses. To ensure immediate availability of this highly effective opioid antagonist, NARCAN is not only available in detentions medical areas and in deputy control stations but detentions deputies are also required to carry NARCAN on their person during their shifts. During calendar years 2020 and 2021 alone, Sheriff's Department employees in the jails responded to 314 incidents of suspected opioid overdose deploying 848 doses of NARCAN and saving countless lives. In conjunction with its community partners, the Sheriff’s Department also makes this lifesaving drug available to incarcerated individuals upon their discharge from Sheriff’s custody.
⑫b. The Number of In-Custody Deaths Experienced by the San Diego Sheriff's Department is Consistent with its Position of Having the Second Highest Number of Total Bookings and Overall Deaths in California Counties
The San Diego Sheriff's Department's position as having the second highest number of in-custody deaths of counties in the state is consistent with its position as having the second highest number of bookings of counties in the state. As demonstrated by Table 1 below, the trend is consistent for at least the top six counties, exhibiting that as the number of bookings goes up, so do the number of in-custody deaths. Additionally, as demonstrated by Table 2 below, as the second most populous county in the state, the County of San Diego also maintains the position as having the second highest number of deaths in the community.
i. Table B is intentionally misleading
The auditors chose to include a table in APPENDIX A which they identify as focusing on two primary categories, "In Custody Deaths and Bookings From 2006 Through 2020." In so doing, they state that the table "presents the rate of deaths per the number of individuals booked in each of the county sheriff's jail systems from 2006 through 2020." They go on to state that "[t]he number of bookings is the total number of individuals who were processed through the jail system." (Emphasis added). However, when the auditors sort the chart, they don't sort it by the column entitled "Total Booked", or even the "Total Deaths" column, both of which would clearly show the correlation between the two (see resorted Table 1 below), but instead they chose to sort by the "Total Deaths per 100,000 Booked" which makes the first three columns appear to have no correlation.
However, the exact same data sorted by the "Total Number of Bookings" column, or the "Total In-Custody Deaths," column clearly shows a correlation between bookings and the number of actual deaths for the six counties with the most bookings in the State of California.
⑬Table 1
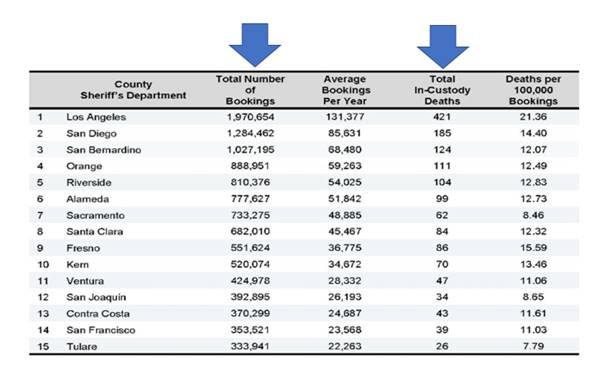
ii. The top 5 counties with the most deaths countywide are also the same
⑫As jails are a microcosm of the communities in which they are located, it should come as no surprise that as deaths in the community increase, deaths in-custody will increase as well. This is particularly true for in-custody deaths due to natural causes, suicide, and accidental deaths due to overdose. As greater numbers of individuals in a community are sick, experience suicidal ideations or are afflicted by substance use disorders, those increased numbers can be expected to replicate themselves in the detention systems serving those communities. As reflected in Table 1 above, the number of in-custody deaths experienced by the Sheriff's Department is not disproportionate to the number of deaths experienced in the San Diego County community regardless of custody status (See Table 2).
⑬Table 2
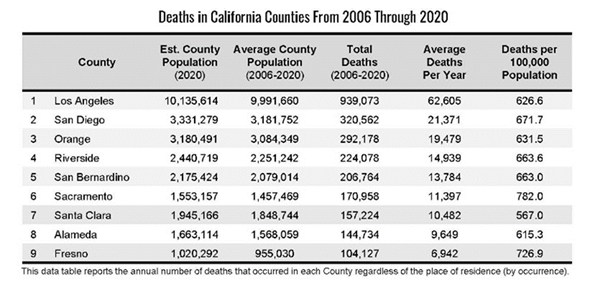
⑭iii. The Comparator Counties Selected by the Auditors Do Not Accurately Reflect the Relevant Peer Group Departments
Considering county size, geographic location and “other factors” the auditors selected the Alameda County Sheriff’s Office, Orange County Sheriff’s Department and Riverside County Sheriff’s Department as comparator departments. From the report, it is unclear how geographic location factored into the selection of the Alameda Sheriff’s Office as a comparator department as the county seats of San Diego County and Alameda County are approximately 490 miles from each other. Similarly, the auditors’ selection of similar counties, based on what appears to be total county population, rather than similar booking numbers is inappropriate. It is unclear how total county population factored into the selection of the Alameda Sheriff's Office as a comparator department when the County of Alameda has less than half the average county population of San Diego County.
The comparator peer group should be based on the total number of individuals encountered (booked) by each department rather than county population. As reflected in Table 3 below, an analysis of the departments, based on total number of bookings, reveals that the statistically relevant departments are the Los Angeles Sheriff’s Department, San Bernardino Sheriff’s Department and Orange County Sheriff’s Department. The San Diego County Sheriff's Department's total bookings for the reviewed 15-year period are within 65% of what the Los Angeles County Sheriff's Department booked for the same period. Similarly, San Bernardino and Orange County Sheriff's Departments booked at least 65% of the total number of bookings that the San Diego County Sheriffs' Department booked.
However, the Riverside County Sheriff’s Department and Alameda Sheriff’s Office, each booked less than 65% of the total number of bookings that the San Diego County Sheriff's Department booked for the same time. By excluding the Los Angeles Sheriff’s Department and San Bernardino Sheriff’s Department, in favor of Riverside County and Alameda County, the auditors excluded the only other departments in the state that booked in excess of 1,000,000 individuals during the audit period. By excluding the Los Angeles Sheriff’s Department and San Bernardino Sheriff’s Department, the auditors also excluded the other two departments with the highest number of in-custody deaths in the state during the audit period in favor of departments having the fifth and sixth highest number of in-custody deaths.
⑬ TABLE 3
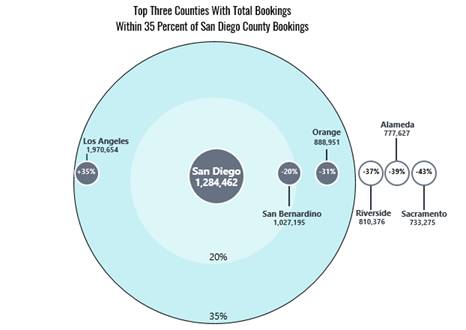
④c. The San Diego Sheriff's Department's Review of In-Custody Deaths Exceeds the Standards Set by the State of California
The Auditor's stated purpose2021-109 AUDIT SCOPE AND OBJECTIVES San Diego County Sheriff’s Department The audit by the California State Auditor will provide independently developed and verified information related to the death of inmates in the custody of the San Diego County Sheriff’s Department (San Diego Sheriff). The audit’s scope will include, but not be limited to, the following activities: 1. Review and evaluate the laws, rules, and regulations significant to the audit objectives. 2. Evaluate the San Diego Sheriff’s policies and procedures on personnel training, facility maintenance and safety, and the provision of health care to inmates. To the extent possible, determine whether these policies and procedures align with minimum standards established through state law and any other applicable guidance. As part of this evaluation, also determine whether any of these policies delay or otherwise impair the ability of medical personnel to provide appropriate medical care to inmates. for the instant engagement is, in pertinent part, to "[e]valuate the San Diego Sheriff’s policies and procedures on personnel training, facility maintenance and safety, and the provision of health care to inmates. To the extent possible, determine whether these policies and procedures align with minimum standards established through state law and any other applicable guidance. As part of this evaluation, also determine whether any of these policies delay or otherwise impair the ability of medical personnel to provide appropriate medical care to inmates." (Emphasis added).
The auditors' findings confirm that the San Diego Sheriff's Department not only meets the minimum standards established through state law and other applicable guidance but, in fact, exceeds those requirements regarding its review of in-custody deaths.
⑮ ④i. The Auditor's Conclusion that the Department's Review of In-Custody Deaths has been Insufficient is Misplaced
The auditors' findings confirm that the Sheriff's Department meets and exceeds the minimum state standards for review of in-custody deaths.
As noted by the auditors, state law requires the Sheriff's Department to conduct a clinical care review within thirty (30) days of every death. The Sheriff's Department meets this requirement by conducting a Mortality/Morbidity Review. The auditors' findings did not reveal any failure on the part of the Sheriff's Department to comply with applicable law with either the timeliness or the substance of the Department's reviews.
Except in the case of a suspected homicide, no other review or investigation is required. In the case of an in-custody death in which homicide is suspected, the Sheriff is statutorily required to investigate the death. That investigation is conducted by the Sheriff's Homicide Unit. The auditors' findings did not reveal any failure on the part of the Sheriff's Department to investigate any in-custody death in which homicide was suspected.
No other reviews by the Sheriff's Department are mandated by state law for in-custody deaths.
While no other reviews are mandated, the Sheriff's Department created and implemented its own multilayer review above and beyond the minimum state standards for review of in-custody deaths.
Although not required for in-custody deaths where homicide is not suspected, the Sheriff's Department, as a matter of practice, conducts an investigation by the Homicide Unit into every in-custody death, not just those deaths where homicide is suspected.
In addition to the Homicide Unit investigation, the Sheriff's Department created its own Critical Incident Review Board (CIRB). The CIRB's role is not limited to reviews of in-custody deaths but includes the review of a variety of critical incidents including uses of force, pursuits, K-9 deployments, overdoses, and other significant events. In-custody deaths due to natural causes are generally not reviewed by the CIRB, unless other issues are identified, as deaths due to natural causes are more appropriately reviewed by the statutorily mandated thirty (30) day Mortality/Morbidity Review conducted by the Department. A further discussion regarding the recommendation that the CIRB review natural deaths is discussed below.
If the CIRB or any member of the Sheriff's Department believes an in-custody death implicates potential misconduct or a failure to meet standards on the part of an employee, the CIRB or any member of the Sheriff's Department can file a Department Generated Complaint requesting that Internal Affairs investigate the matter.
Penal Code section 832.5 requires every law enforcement agency in the state to establish a procedure to investigate complaints lodged by members of the public against personnel of the agency. In addition to investigating complaints from members of the public, the Sheriff's Department investigates "department generated" complaints, which can be lodged by any member of the department, in the same manner as it investigates a complaint by a member of the public. If there is potential misconduct or a failure to meet standards on the part of an employee related to an in-custody death, the Sheriff's Department does not wait for a member of the public to file a complaint but can and does initiate an Internal Affairs investigation based on a department generated complaint.
As the auditors' findings make clear, the reviews conducted by the Sheriff's Department not only meet the minimum standards established by the state, the multilayered approach adopted by the Sheriff's Department far exceeds those minimum standards. Any deficiencies in the state's minimum standards regarding the review of in-custody deaths is most appropriately addressed to the Legislature and/or the BSCC, not to the Sheriff's Department as the audited entity.
⑯ii. The Critical Incident Review Board's Roles of Preventing Future Litigation and Improving the Health and Welfare of Incarcerated Individuals are Not Mutually Exclusive
The auditors stated there should be more transparency regarding the process and findings of the Sheriff's CIRB Board. The CIRB reviews occur within the confines of the attorney-client relationship and are not reported out publicly. Every governmental entity, even those such as the State Legislature or a Board of Supervisors, both of which are subject to the Brown Act's open meeting requirements, are afforded the opportunity to engage in candid conversations with its counsel within the confines of the attorney-client relationship.
Notwithstanding the auditors' particular concern regarding the existence of the attorney-client privilege, the CIRB's role of preventing future litigation compliments rather than undercuts the Department's goal of improving the health and welfare of incarcerated individuals entrusted to the care and custody of the Sheriff. As items of concern are identified during a critical incident, such as an in-custody death, the CIRB review is focused with an eye towards what changes have already been implemented by the chain of command to remedy any deficiencies before the matter made it to the CIRB for review, as well as any changes the chain of command may not have already identified and/or implemented to minimize the risk of a recurrence. If the CIRB identifies any best practices or changes not previously identified and implemented by the chain of command prior to its review, the CIRB is empowered to make such recommendations.
As it relates specifically to in custody deaths, the CIRB concentrates not only on the death itself, but also considers the handling of the inmate from the time the inmate was originally booked. The Board looks to determine whether any warning signs existed, whether appropriate and timely safety checks occurred, and whether there were any risk reduction lessons that could be derived from the incident.
While the focus of the CIRB may be risk management, the mechanism by which risk management is ultimately accomplished is clearly through the promotion of best practices and policies that improve the health and welfare of incarcerated individuals and holding staff accountable.
While the Auditor was "particularly concerned" that the Sheriff's Department does not publicly report out its CIRB discussions, all Sheriff's Department policies, procedures, training, and education materials are published on the Sheriff's Department's website. Any changes to Sheriff's policies, procedures, training, or education, whether recommended by the CIRB or implemented by management prior to or without the need for a CIRB review, are published and available for the public to access on the Sheriff's Department's website. In addition to the attorney-client privileged nature of the CIRB discussions, the Sheriff's Department would also be prohibited by state statutory and constitutional privacy considerations from disclosing any discussions by the CIRB regarding employee misconduct or Internal Affairs investigations.
⑰d. In Addition to Its Own Internal Reviews, the Sheriff’s Department is Already Subject to Independent Oversight by Multiple External Organizations
④Local detention facilities are subject to a myriad set of regulations and laws based on statutory law, constitutional guarantees, and case law. In order to ensure county detention facilities, comply with these requirements, the BSCC promulgates regulations under Title 15 of the California Code of Regulations, establishing statewide standards for detention facilities. In order for facilities to maintain their certification to operate, counties are subject to bi-annual inspections by the BSCC. The auditors' findings confirm that the Sheriff’s Department meets the standards established by the BSCC under Title 15.
In addition to the bi-annual inspections by the BSCC, pursuant to its authority under Penal Code section 919, the San Diego County Grand Jury conducts an annual inspection of the Sheriff’s Department detention facilities.
The San Diego County Citizens Law Enforcement Review Board, pursuant to its County Charter authority, is also empowered to, and does, investigate in-custody deaths.
⑰e. In its continuing efforts to enhance medical and mental healthcare, and exceed the standards set by the State of California, the Sheriff’s Department engaged reviews by multiple separate external entities specializing in correctional healthcare
The Sheriff’s Department was reviewed by two entities in pursuit of enhancing system operations related to medical and mental health care. These included a look at suicide prevention practices by nationally recognized expert, Mr. Lindsay Hayes, and a preliminary review by the National Commission on Correctional Healthcare (NCCHC). Both entities produced reports for the Sheriff's Department that have been used to enhance policies and procedures to align with best practices and meet recommendations. The reports are available on the Sheriff's Department public website at www.sdsheriff.gov.
⑤III. Recommendations
a. Intake Screening
CSA Recommendation:
Revise its intake screening policy to require mental health professionals to perform its mental health evaluations. These evaluations should include a mental health acuity rating scale to better inform individuals' housing assignments and service needs while in custody. The Sheriff's Department should communicate the acuity rating as it assigns to individuals to all detentions staff overseeing them.
The Sheriff's Department concurs with the auditor's assessment that Qualified Mental Health Providers (QMHP) are the more appropriate staff to conduct the mental health screening portion of the intake process. The Medical Services Division (MSD) received funding for additional staffing in July 2021 and is currently in the process of recruiting and hiring from a limited pool of candidates. Additional staffing will allow us to provide a comprehensive screening process utilizing the electronic health record, in accordance with National Commission for Correctional Health Care (NCCHC) standards. Some identified QMHP staffing duties would be to conduct the Behavioral Health (BH) screening, complete a risk/needs assessment, to include substance use disorder (SUD). The assessment would determine a behavioral health acuity rating, schedule psychiatric appointments, schedule follow up QMHP appointments, assess for the need of placement into our Inmate Safety Program (ISP) and obtain Release of Information authorizations. QMHPs and nursing staff working in collaboration at the initial intake assessment and throughout a patient's incarceration promotes a comprehensive whole person model of care.
Ongoing effective communication between medical staff and sworn staff is paramount in ensuring the safety and wellbeing of our patients. Our plan is to implement bidirectional communication with our Jail Information Management System to ensure sworn staff are aware of the mental health recommendations. All staff are responsible for the appropriate and timely care of our patients. Further analysis will need to be done to evaluate the impact this acuity rating system would have on our system of jail classification and housing needs.
CSA Recommendation:
Create a policy requiring health staff to review and consider each individual's medical and mental health history from the county health system during the intake screening process.
San Diego County does not have an interconnected health information exchange. Hospital centers and medical systems independently manage their data systems and may or may not voluntarily participate or contribute to a health information exchange. Our health staff currently have access to the following county databases:
i. Health and Human Services Agency – Cerner Community Behavioral Health (CCBH)
Cerner Community Behavioral Health is a behavioral health-specific electronic health record that specializes in the delivery of community mental health, inpatient mental health, outpatient mental health, substance use disorder and developmental disabilities care. Although there may be some patients who are not in the database and do not have data entered, we continue to review and enter data referencing our patient encounters while in our care.
As of April 2021, all QMHPs (mental health clinicians, psychologists, psychiatrists, psychiatric technicians) have "read" access to Cerner Community Behavioral Health (CCBH). QMHPs can review records at any point in the patient's stay. The planned integration of a QMHP into the intake process for behavioral health screening will fulfill this recommendation. In addition to having access to review community behavioral health records, the Sheriff's Detention Services Bureau contributes to this community database by recording and entering mental health care provided while the patient is in our custody as part of the county's continuum of care. The Sheriff's Medical Services Division intends to adhere to the NCCHC standards for the referral process.
ii. Health and Human Services Agency – San Diego Immunization Registry
The San Diego Immunization Registry (SDIR) is a County system that offers Sheriff's Department health staff the ability to verify a patient's vaccination status. SDIR is limited to vaccinations given in San Diego County. If a patient receives an immunization outside of San Diego County or opts to "lock" their record, health staff will not have the ability to verify vaccination status. Currently we have sufficient access to SDIR.
iii. San Diego Health Connect
San Diego Health Connect was originally designed to allow for medical information to be exchanged between community clinics. The database only covers medical (not mental health/behavioral health issues) and each patient must consent to participate. Very few patients are registered in the system, and the system is undergoing restructuring.
b. Medical & Mental Health Follow-Up
CSA Recommendation:
Revise its policy to require that nurses schedule an individual for an appointment with a doctor if that individual has reported to the nurse for evaluation more than twice for the same complaint.
The Sheriff's Department concurs with the auditors' assessment that a revision is necessary to address the process for medical/mental health referral after two requests. The Sheriff's Medical Services Division intends to implement a health care requests and services process in accordance with NCCHC standards. Patients will be referred to a provider to be evaluated. When a patient presents for health care services more than two times with the same complaint and has not seen a provider, they will receive an appointment to do so. Some mental health patients need assistance with advocating for their medical care. Regular follow-up and ongoing engagement with QMHPs is essential to identifying patients who face these challenges.
CSA Recommendation:
Revise its policy to require that a nurse perform and document a face-to-face appraisal with an individual within 24 hours of receipt of a request for medical services to determine the urgency of that request. Revise its policy to require that a member of its health staff witness and sign the refusal form when an individual declines to accept necessary health care.
The Sheriff's Department concurs a timely medical response to patient concerns is extremely important, and that repetitive patient refusals or an abject delay in follow-on scheduling of medical care are concerning issues and could potentially precipitate an adverse condition or event. We are committed to the health and well-being of our patients, and are developing safeguards to ensure a timely, efficient re-engagement of both medical and mental health services.
The Sheriff's Department is currently focused on a more nursing centric model. For health staff, we are in the process of embedding nursing staff at the ward level, assigning nursing staff to most housing units in support for the Primary Care nursing model. Nurses will be there to perform face-to-face assessments of their assigned patients (on the floors and during sick call) and involved in counseling and advocacy efforts for every refusal. We have worked with our contracted medical providers to develop daily rounds in designated modules to address acute and ongoing assessments for specified patients. We continue to pursue accreditation from the NCCHC which requires a face-to-face assessment withing 24 hours of a medical request being filed (NCCHC Standards J-E-07).
CSA Recommendation:
Revise its policy to require more frequent psychological follow up after release from the inmate safety program to at least monthly check-ins.
The Sheriff's Department will reevaluate our policies on psychological follow-up. Our current Inmate Safety Program policy reflects the recommendations from Mr. Lindsey Hayes regarding our follow up protocol. Mr. Hayes is nationally recognized as an expert in the field of suicide prevention within custodial settings and has served as a Federal Court Monitor. While placement into any of our Inmate Safety Program specialized housing requires a mental health response and establishes a basis for continued follow-up; the Sheriff's Department's current planned expansion and hiring of additional mental health professionals will allow for more frequent encounters and the investment of time necessary for higher quality mental health care.
⑱Mr. Hayes specifically states, "it is recommended that the follow-up schedule be simplified and revised as follows: follow-up within 24 hours, again within 72 hours, again within 1 week, and then periodically as determined by the clinician until release from custody." As a nationally recognized expert, SDSD has adhered to Mr. Hayes' recommendation.
c. Safety Checks
CSA Recommendation:
Revise the safety check policy to include the requirement for staff to check that an individual is still alive without disrupting the individual's sleep.
The Sheriff's Department will reevaluate current policy and incorporate best practices. SDSD is exploring technologies to assist with monitoring a "proof of life" for all incarcerated individuals with minimal sleep interruption through staff contact. The Sheriff's Department is evaluating industry capabilities, and in the process of developing a more robust facility Wi-Fi system capable of supporting technological advancements in monitoring the welfare of our population. The Sheriff's Department's planned integration of Bodyworn Cameras (BWC) into the custodial setting will greatly assist in showing the point of view each deputy has during the safety checks.
CSA Recommendation:
Develop and implement a policy requiring that designated supervising sworn staff conduct audits of at least two randomly selected safety checks from each prior shift. These audits should include a review of the applicable safety check logs and video footage to determine whether the safety checks were performed adequately. In addition, the policy should require higher-ranking sworn staff to conduct weekly and monthly audits of safety checks. The policy should also require each facility to maintain a record of the safety check audits that staff perform.
Sheriff's Department line supervisors conduct electronic log reviews every shift. This review includes ensuring the timeliness of safety checks in accordance with established Policy & Procedures. The Sheriff's Department's current practice requires supervisors conduct video audits of random safety checks and will formalize this into policy.
d. Sworn Discovery of Medical Emergency
CSA Recommendation:
Revise its policies to require that sworn staff members immediately start CPR without waiting for medical approval, as safety procedures allow.
⑲Sworn staff does not require approval from medical to start CPR. Current DSB P&P M.5 I.B. states, "When the severity of the medical emergency requires it, and as soon as it is safe to do so (unless death is obvious, such as decapitation, obvious rigor mortis, etc.), deputies acting as first responders will provide basic life support and first aid. Upon arrival, facility health staff will assess the severity of the inmate’s injury/distress, provide first-aid, and may assist or take over cardiopulmonary resuscitation (CPR) responsibilities as directed and/or needed." This policy in its current form has been in effect since January 2012.
The Sheriff's Detention Services Bureau In-Service Training Unit distributed a training bulletin on Signs of Medical Distress and Life-Threatening Emergencies on June 18, 2021. The purpose of the training bulletin was to familiarize staff with signs of death or near death and appropriate actions of sworn staff when observing such signs of medical distress. Per DSB Policy and Procedure section M.6, "Any life-threatening medical emergency shall trigger a 911 request for a paramedic emergency response team. Sworn and health staff shall initiate emergency response and basic lifesaving measures until relieved by the paramedic emergency response team."
e. In-Custody Death Follow-Up
Staff will provide a written report of each 30-day medical review to its management.
The Sheriff's Department concurs with this recommendation.
CSA Recommendation:
When warranted, the report should specify recommendations for changes to prevent future deaths.
The Sheriff's Department concurs with this as it relates to the perspective of the Chief Medical Officer or the Director of Mental Health's review of the case.
CSA Recommendation:
The 30-day medical review should determine the appropriateness of clinical care; assess whether changes to policies, procedures, or practices are warranted; and to identify issued that require further study.
The Sheriff's Department concurs with this as it relates to the perspective of the Chief Medical Officer or the Director of Mental Health's review of the case. There are other processes currently in place to look for policy, training, or accountability issues following critical incidents.
f. Critical Incident Review Board
CSA Recommendation:
Revise its policy to require that the Critical Incident Review Board review natural deaths.
In July of 2021, the Division of Inspectional Services (DIS), Sheriff's Legal Affairs, and CIRB board members evaluated potential updates to policy and procedures section 4.23 – Department Committees and Review Boards. This assessment included reviewing in-custody deaths deemed natural by the Medical Examiner's Office, as the auditors recommend. This, along with other changes are anticipated to be in a pilot phase beginning February 2022. Historically, if a natural death is deemed to have potential issues of any nature it may be presented to CIRB at the discretion of the board members. Also, the Chief Medical Officer and appropriate medical staff conduct a mortality/morbidity review of each in-custody death for their determination of any changes that are needed related to medical care for incarcerated individuals.
CSA Recommendation:
Require the Sheriff's Department to make public the facts it discusses and recommendations it decides upon in the Critical Incident Review Board meetings to establish a separate public process for reviewing deaths and making necessary changes.
⑯CIRB presentations allow the Sheriff's legal advisor and the various commands the ability to review critical incidents to identify issues that should be addressed in various areas, including, but not limited to, training, policies, procedures, staffing, and equipment. The confidential environment provided by the CIRB is essential to the free exchange of ideas, and concerns, in anticipation of future litigation because of a given incident, and in order to avoid future litigation through implementation of best practices. Effectiveness and thoroughness of presentations would likely be diminished if the attorney-client privilege is removed, or information is required to be disclosed during pending, or anticipated litigation. Much of the information presented in CIRBs is intended for individuals who have a vast familiarity and understanding of law enforcement or detention operations, department policies, and state and federal laws, and may contain confidential information including criminal history, medical history, and peace officer personnel records.
g. Citizen's Law Enforcement Review Board Integration
CSA Recommendation:
Revise its policy to include CLERB in its immediate death notification process.
Revise its policy to allow a CLERB investigator to be present at the initial death scene.
The Sheriff's Department is currently evaluating a process to integrate the CLERB investigator into the initial notification and response to in-custody deaths, to include a scene walkthrough and incident brief.
CSA Recommendation:
Revise its policy to encourage its staff to cooperate with CLERB's investigations, including participating in interviews with CLERB's investigators.
⑳The CLERB has subpoena powers for in person sworn staff interviews. In 2003, the CLERB discontinued issuing Sheriff's Department sworn staff interview subpoenas and opted for written responses due to Public Safety Officers Procedural Bill of Rights (POBAR) conflicts where ultimately the interviews did not benefit the CLERB's investigations. The CLERB continues to have subpoena powers. This recommendation should be re-directed to the CLERB for its review to change its current practice and exercise its authority to issue subpoenas to Sheriff's sworn staff.
⑤IV. Conclusion
The Sheriff's Department takes seriously its responsibility to maintain a safe and healthy environment in the county jails.
⑰The Sheriff’s Department has welcomed and consistently made itself available for, and cooperated with, reviews by numerous entities including the Disability Rights California, Lindsay Hayes, the NCCHC, the San Diego County Grand Jury, and the Citizens Law Enforcement Review Board. We did the same with the California State Audit. After every review, the Department seriously considers every recommendation and implements those that are appropriate and possible, given existing laws, infrastructure, staffing limitations, and best practices. During the 15-year audit period the Department has taken numerous steps towards providing the best care for those detained in the jail system. To date, the following improvements have been made:
- Changing our pharmacy business processes
- Implementing a new electronic health record system
- The continuous review and updates to both Detentions Services and Medical Services policies and procedures.
- Increased medical service provider coverage
- Enhanced communication and collaboration between medical and sworn staff which includes the:
- Implementation of a medical "scene manager" to ensure relevant communication during critical incidents
- Issuance of facility communication equipment in the nursing stations to expedite response
- Development of collaborative training between sworn and health staff related to health emergencies
- Developing and mandating an 8-hour suicide prevention training and a 2-hour refresher training
- Enhancing our suicide assessment and monitoring
- Enhancing the continuity of care for inmates removed from suicide precautions; and
- Enhancing the quality assurance process for intake screening related to suicide prevention
We recognize that we cannot rest on the things that we have done. As the Sheriff’s Department shared with the auditors, the Department is pursuing accreditation by the National Commission on Correctional Health Care (NCCHC). The Sheriff’s Department currently meets the standards established by the State of California, final accreditation by the NCCHC would add yet another layer of continuing, independent, external oversight. However, our goal is to exceed all standards. We strive to provide a better than community standard in the medical and mental health care of incarcerated individuals.
The San Diego Sheriff's Department recognizes that comparisons will be made among counties in California. We regularly confer with other counties in the state and across the country to identify best practices. We remain focused on what we can improve and are committed to do so. It is with this attitude that the San Diego County Sheriff's Department will go forward in assessing the recommendations made by the auditor in the draft report.
Sincerely,
William D. Gore, Sheriff
Comments
California STATE AUDITOR’S COMMENTS ON THE RESPONSE FROM THE SAN DIEGO COUNTY SHERIFF’S DEPARTMENT
To provide clarity and perspective, we are commenting on the Sheriff Department’s response to our audit. The numbers below correspond to the numbers we have placed in the margin of the Sheriff’s Department’s response. In certain areas of its response, we have summarized our comments according to the respective sections in its response rather than comment on all of the individual areas of its response that we believe are deficient or misleading.
①We provided the Sheriff’s Department five business days to review and provide a formal response to the draft audit report, which is our standard practice for all audited entities. As part of our audit process and in accordance with generally accepted government auditing standards, we also met with the staff of the Sheriff’s Department, including the Sheriff and other executive management personnel, on numerous occasions during the audit to ensure they were fully briefed on our findings, conclusions, and recommendations.
②We have redacted portions of the Sheriff’s Department’s response containing information that is deliberative in nature or reflects confidential discussions not used in support of the audit report. Additionally, some of the redacted text contains excerpts from the draft report. In accordance with Government Code sections 6254, 8545, and 8545.1, it was necessary for us to make these redactions to protect our confidential work and because the improper disclosure of draft audit documents is a misdemeanor.
③The Sheriff’s Department states that the highly redacted version of the draft report made it difficult for it to submit a meaningful, comprehensive response. On the contrary, the report that we provided contained all findings, conclusions, and recommendations pertaining to the Sheriff’s Department—all of which we had previously shared with its management on numerous occasions. The sections we redacted pertained to other audited entities, such as CLERB, which were not relevant for the Sheriff’s Department’s response. Further, because state law makes it a crime to improperly disclose ongoing audit information, when the California State Auditor’s Office sends draft sections of an audit report to an audited agency for its comment, we redact from the draft those provisions that concern the other agencies being audited. Moreover, the Sheriff’s Department misunderstands the purpose of an audit report, which is to summarize the results of our audit work that the Audit Committee directed us to perform. Our working papers contain the documentation and analyses that support the findings, conclusions, and recommendations in the audit report. Additionally, Government Code section 8545, prohibits the public release of any work papers pertaining to an audit that has not yet been completed. Until the audit report is published, we are required to hold any supporting work papers in strict confidence.
④Although we concluded that the Sheriff’s Department’s policies generally align with BSCC standards, we found significant deficiencies that we discuss throughout the report. Moreover, BSCC designs the standards to be a minimum that all counties can achieve, regardless of variation in resources at the local level. However, we found that BSCC’s approach enables counties that house large numbers of incarcerated individuals to provide lower levels of care. Therefore, to improve the level of care in local detention facilities, we made recommendations to address weaknesses in the Sheriff’s Department’s policies and procedures as well as in BSCC’s standards.
⑤The Sheriff’s Department’s concerns related to our findings and conclusions contradicts its agreement with our recommendations. Under generally accepted government auditing standards, which we are required to follow, the findings and conclusions of an audit form the basis for recommendations.
⑥The Sheriff’s Department incorrectly states that we do not comply with audit standards, which it asserts here. We conducted this audit in accordance with generally accepted government auditing standards, which we are required to follow, and the California State Auditor’s thorough quality control process. In following audit standards, we are required to obtain sufficient and appropriate audit evidence to support our conclusions and recommendations. As with all of our audits, we engaged in extensive research and analysis for this audit to ensure that our report presented a thorough and accurate representation of the facts, and included all relevant information. We stand by the statements in our report, which are based on sufficient and appropriate evidence. Further, as with all of our audits, our public report includes the required statement indicating that we performed this audit in compliance with audit standards.
Moreover, as part of our adherence to audit standards, our staff possess the collective knowledge, skills, and abilities to conduct performance audits, including those of local law enforcement entities.
⑦The Sheriff’s Department’s comments questioning the accuracy of our report are unfounded. The high rate of deaths in San Diego County’s jails compared to other counties raises concerns about underlying systemic issues with the Sheriff’s Department’s policies and practices. Throughout Chapter 1 we provide numerous examples of deficiencies in the department’s policies and procedures that likely contributed to the deaths of some incarcerated individuals and how these policies and procedures do not align with certain best practices used by comparable counties and other entities. Specifically, we describe how the Sheriff’s Department did not consistently follow up with individuals who needed medical and mental health services, and that lack of attention may have contributed to their deaths. Finally, although the Sheriff’s Department indicates that our audit does little to document or provide context of its efforts to respond to deaths, we describe the improvements the Sheriff’s Department has made. Because we found that weaknesses continue to exist in the Sheriff’s Department’s policies and procedures, we made recommendations to address those weaknesses.
⑧Because the Sheriff’s Department’s response included specific details about an in‑custody death, such as the case number and a more detailed description of the incident, we redacted this text because it contained confidential information and to protect the privacy of the individuals involved. We clarified our report to make it clear that our concern in this case is related to timeliness of its response to the emergency and not the issue of who provided CPR.
⑨The Sheriff’s Department incorrectly states that it was not given information about the Alameda Sheriff’s Office, the Orange Sheriff’s Department, and the Riverside Sheriff’s Department. The draft report that we sent to the San Diego Sheriff’s Department contained primarily publicly available information for these counties to provide context for the Sheriff’s Department’s findings.
⑩When multiple entities are examined in an audit, the California State Auditor’s Office is required under state law to maintain confidentiality with each of those entities. Maintaining confidentiality among multiple subjects of an audit is essential to ensuring the integrity and quality of the evidence upon which the audit’s conclusions are based. Moreover, based on its misunderstanding of state law, the Sheriff’s Department wrongly asserts that our office was required to provide it with supporting documentation pertaining to other auditees because they are public records. Government Code section 8545 prohibits the public release of any work papers or documents pertaining to an audit that has not yet been completed. Until the audit report is published, any supporting documents are held in strict confidence.
⑪The Sheriff’s Department’s concern regarding which version of policies and procedures we based our findings on is unfounded. Our analysis included identifying the policies applicable at the time of the incident we reviewed and determining whether they were subsequently updated to address our concerns. For example, we identified a weak policy for mental health services that contributed to an individual’s death by suicide and determined that the Sheriff’s Department subsequent revision to that policy did not fully address our concerns.
⑫The Sheriff’s Department’s approach does not allow for a fair comparison between counties. In Table A.2, we present the rate of in‑custody deaths based on the relative size of 15 counties. We believe that this objective presentation allows a reader of the report to compare the counties in a more meaningful way. Nevertheless, in both presentations, the Sheriff’s Department is among the highest in number and rate of deaths in its jails.
⑬Table 1, Table 2, and Table 3 on pages 98 to 100 were created by the Sheriff’s Department and are not part of our report. We do not attest to the accuracy of the information the Sheriff’s Department presents.
⑭We stand by our selection of the comparable counties referenced in our audit. As we state in the Scope and Methodology, we selected these counties considering relative size, geographical location, and other factors. We also used professional judgement in selecting a large county in a different region to obtain broad perspective. Our selection of counties satisfied the audit objectives and resulted in sufficient and appropriate evidence to support our findings, conclusions, and recommendations.
⑮We stand by our conclusion that the Sheriff’s Department’s reviews of in‑custody deaths are insufficient. The Sheriff’s Department did not sufficiently document the results or recommendations from its 30‑day medical reviews. For 22 of the 30 cases we reviewed, the Sheriff’s Department was unable to provide us with documentation from these reviews that detailed any findings or conclusions about the clinical care given, identified whether any concerns required further study, or stated whether changes to policies, procedures, or practices are warranted. We believe that if the Sheriff’s Department properly documented the 30‑day medical reviews, it could better identify and track instances when it did not provide sufficient medical and mental health follow‑up care before an individual’s death, such as those we discuss in Chapter 1.
Further, the Sheriff’s Department does not complete internal affairs investigations related to in‑custody deaths frequently enough for it to provide significant value. The small number of these investigations related to deaths—coupled with the lack of meaningful changes arising from the Critical Incident Review Board meeting and the 30‑day medical review—calls into question the Sheriff’s Department’s commitment to protecting individuals in its custody.
⑯The Sheriff’s Department mischaracterizes our point about its Critical Incident Review Board. To clarify, the stated purpose of the board is to consult with the department’s legal counsel when an incident occurs that may give rise to litigation. Therefore, it appears that its primary focus is protecting the Sheriff’s Department against potential litigation rather than focusing on improving the health and welfare of incarcerated individuals.
Further, after the board meets to discuss in‑custody deaths, it has not always taken meaningful action to prevent deaths, even when it identifies problems with its policies and practices. Specifically, even though the board discussed critical issues in some meetings, it did not always make recommendations for addressing these issues.
Moreover, although we do not disagree with having a confidential forum to discuss potential litigation matters, we are concerned that the Sheriff’s Department does not have a separate public process to demonstrate that it is addressing deficiencies in its policies, procedures, and practices after in‑custody deaths occur. By keeping its findings and recommendations confidential, the department risks conveying to the public that it is not taking these deaths seriously, investigating them thoroughly, or acting to prevent future incidents. Further, the Sheriff’s Department is disingenuous in its response that it provides all changes to policies, procedures, training, or education on its website. The policies posted on its website do not communicate changes it made in response to in‑custody deaths. Having its policies available online in their entirety without specifically identifying those changes that it made in response to in‑custody deaths is not transparent in this respect.
⑰Even though the Sheriff’s Department was reviewed by external entities, it has failed to implement key recommendations from external entities, including recommendations from the San Diego County Grand Jury, CLERB, Disability Rights California, and a suicide prevention consultant. Some of the recommendations that the Sheriff’s Department failed to implement are related to weaknesses in its policies and procedures that we identify in this report. Accordingly, we are concerned about whether the Sheriff’s Department will make meaningful changes to address these systemic weaknesses.
⑱The timeframes that the Sheriff’s Department refers to are unrelated to our recommendation. Our recommendation is for the Sheriff’s Department to update the minimum ongoing follow-up in its policy from 90 days to at least monthly. Reports and studies related to mental health indicate that more frequent psychological follow‑up, such as check‑ins performed weekly rather than every 90 days, leads to faster recovery and is more effective for individuals with mental health needs.
⑲Although the Sheriff’s Department asserts that its current policy appropriately addresses safety concerns regarding sworn staff administering CPR to incarcerated individuals, we had concerns with this policy during our audit. In some instances, sworn staff did not perform or delayed lifesaving measures because they thought the individual was dead. However, when department medical staff arrived minutes later, they immediately began lifesaving measures on the individual, including CPR. This fact calls into question the ability of sworn staff to assess whether unresponsive individuals might benefit from such potentially lifesaving measures.
⑳We explain our concerns with CLERB not directly interviewing sworn staff. Our recommendation to the Sheriff’s Department to encourage its staff to cooperate with CLERB’s investigations aligns with our recommendation to CLERB.